Downloaded 34 times













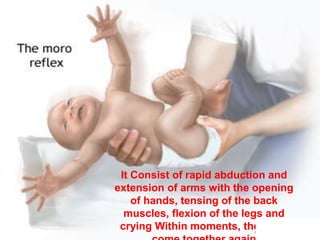


















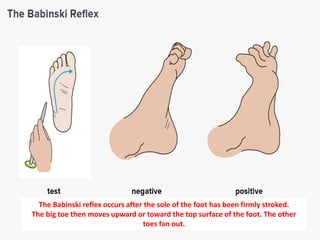



























This document discusses various reflexes in infants and their clinical significance. It describes several reflexes like the moro, palmar, plantar, and babinski reflexes. These reflexes are present at different gestational ages and disappear at varying times as the infant develops. The presence, absence, strength, or persistence of certain reflexes beyond the normal period can provide clues about an infant's neurological development and identify potential abnormalities. Reflexes also help assess an infant's motor development and skill progression.