This document provides an overview of pulmonary embolism (PE). It discusses the historical context, pathophysiology, risk factors, clinical presentation, diagnostic testing and treatment of PE. Some key points include:
- PE is a common cause of preventable death, with over 600,000 cases annually in the US.
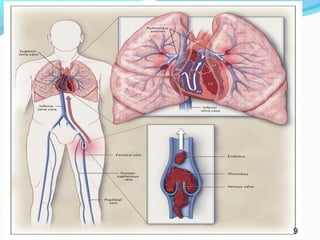
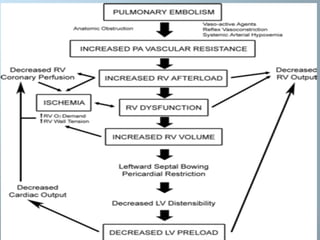
- Virchow's triad of hypercoagulability, stasis, and endothelial injury contributes to the development of PE.
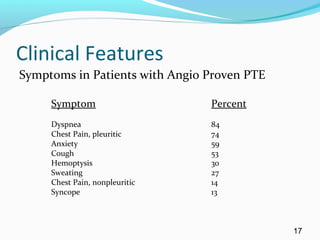
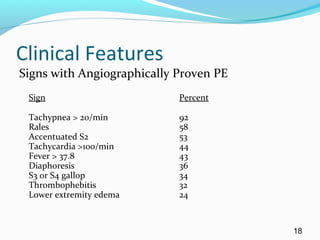
- Clinical presentation is often nonspecific, and the classic triad of symptoms occurs in less than 20% of cases.
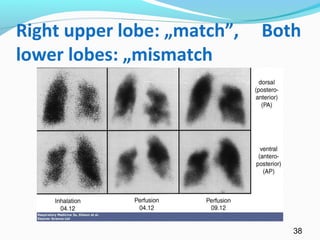
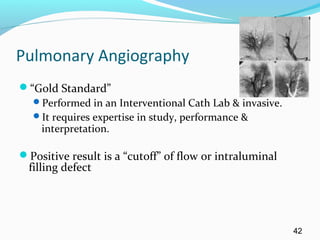
- Diagnostic testing includes D-dimer, chest CT, ventilation-perfusion scanning and pulmonary angiography. Early treatment with antico