

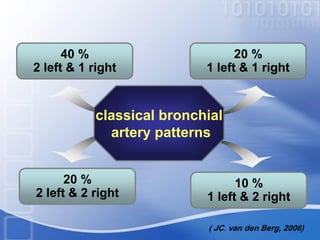
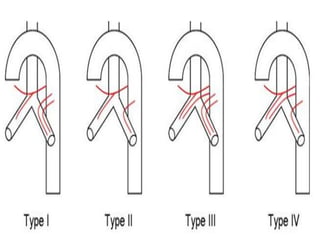
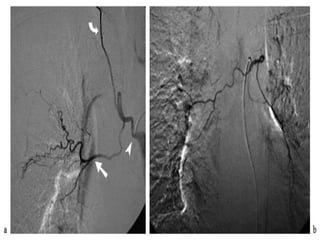
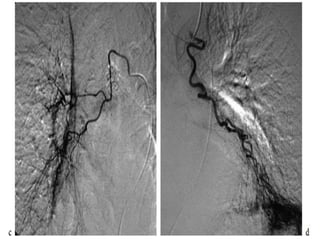


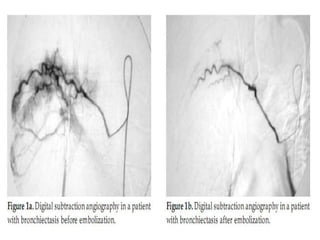
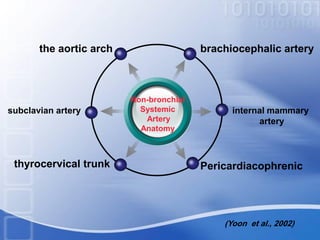

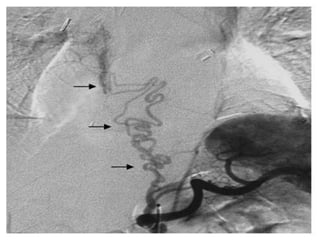





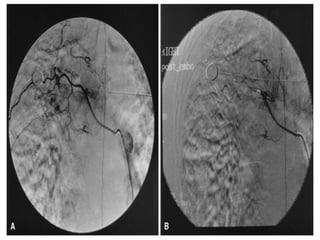

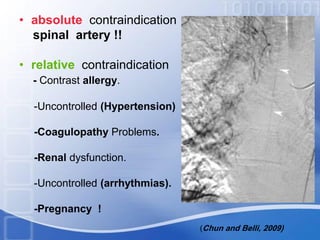







This document discusses embolotherapy for massive hemoptysis. It defines massive hemoptysis and outlines the evaluation and causes. Bronchial artery embolization is presented as the most effective nonsurgical treatment, with short-term success rates of 77-99% and long-term success possible with repeat embolization and controlling underlying disease. The document reviews bronchial artery anatomy, various embolization agents like particles and coils, the embolization procedure and potential complications.























































































