Downloaded 657 times
































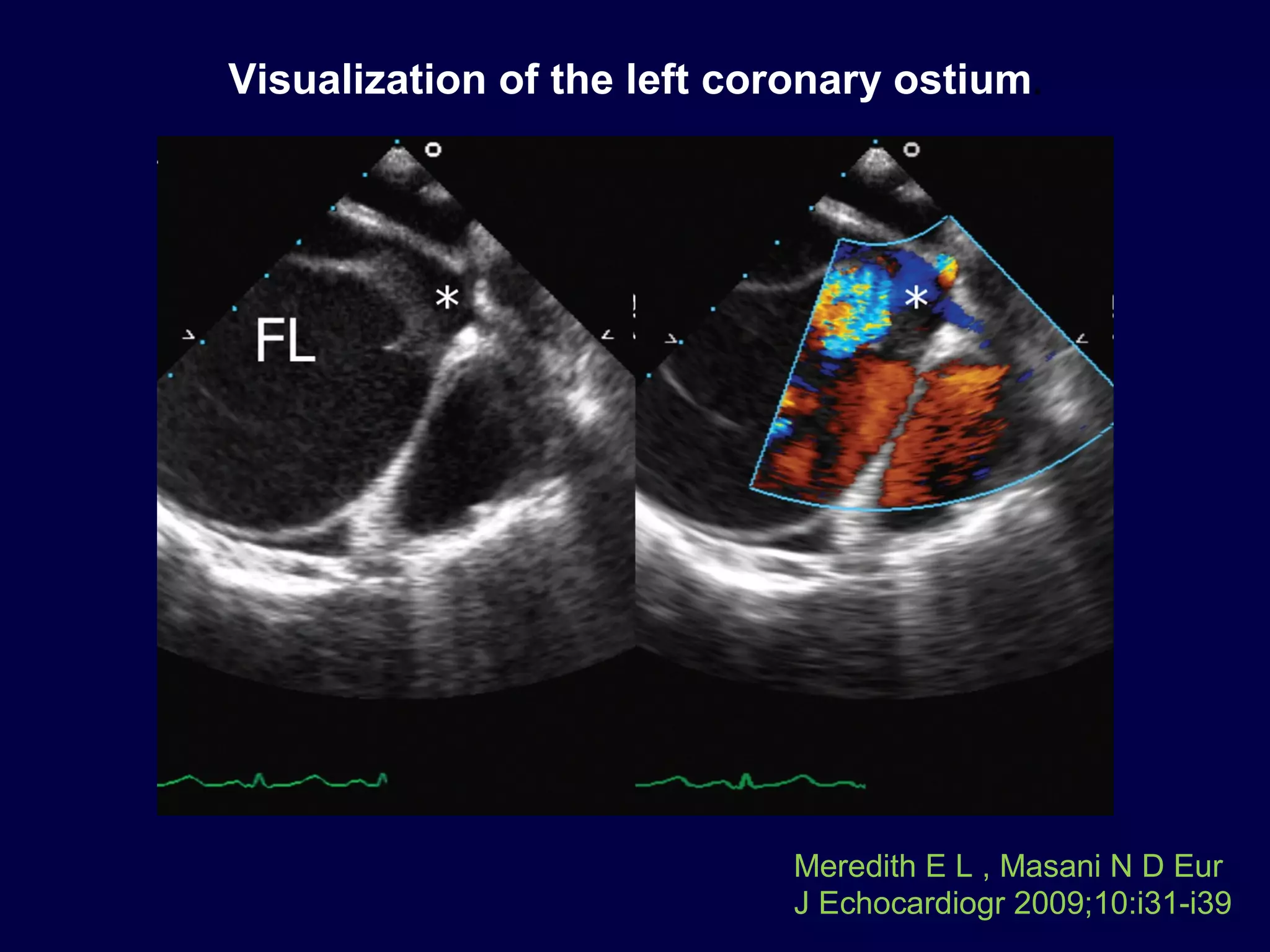



































The document discusses various diseases of the aorta including aortic dissection, intramural hematoma, penetrating atherosclerotic ulcer, aortic aneurysm, atherosclerotic disease, coarctation, and aortic trauma. It provides an overview of the anatomy, clinical presentation, diagnostic imaging, complications, and treatment options for each condition. Key imaging modalities for diagnosis include transthoracic echocardiography, transesophageal echocardiography, CT, and MRI. Mortality rates and predictors of outcome are also reviewed.























































































