Downloaded 1,731 times












![Clinical features
Sudden onset of unliateral pleuritic chest pain
Breathlessness
[In pts with a small pneumothorax, physical
examination may be normal ]](https://image.slidesharecdn.com/pneumothorax-141022120943-conversion-gate02/75/Pneumothorax-15-2048.jpg)





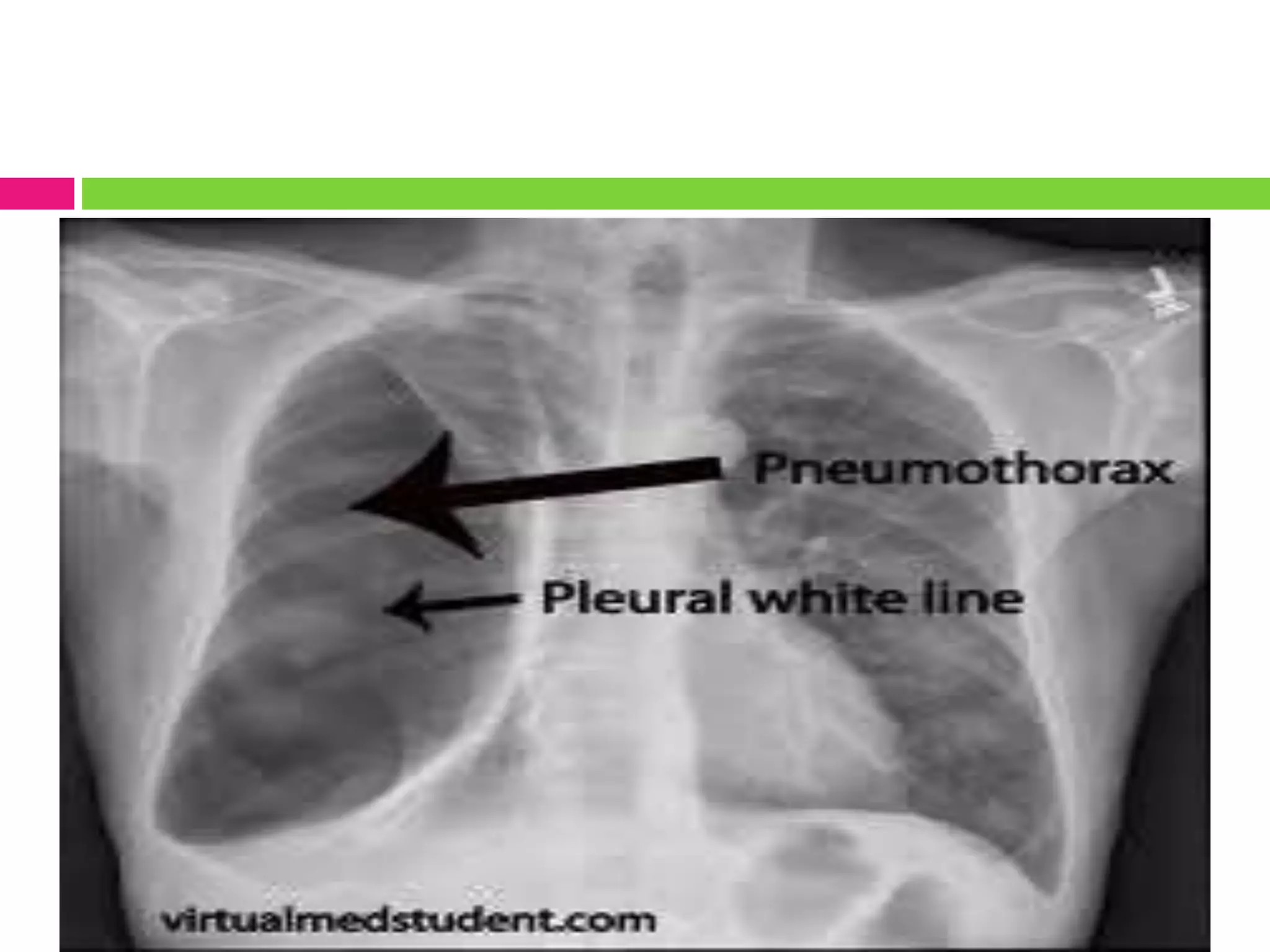
![Investigations
Chest x ray
Shows : increased radiolucency, with absence of
bronchovascular markings
extend of mediastinal shift.
pleural fluid ,if present .
underlying pulmonary disease .
(costophrenic angles are clear)
[care must be taken to differentiate b/n a large pre-existing bulla &
a pneumothorax to avoid misdirected attempts at aspiration]](https://image.slidesharecdn.com/pneumothorax-141022120943-conversion-gate02/75/Pneumothorax-22-2048.jpg)






![Secondary pneumothorax
Even a small secondary pneumothorax may
cause respiratory failure, so all such patients require
↓
Intercostal tube drainage
[Intercostal drains are inserted in the 4th ,5th or 6th
intercostal space in the midaxillary line ,connected
to an under waterseal]](https://image.slidesharecdn.com/pneumothorax-141022120943-conversion-gate02/75/Pneumothorax-30-2048.jpg)





Pneumothorax is the presence of air in the pleural space and can be spontaneous, due to trauma, or iatrogenic. It is classified as primary spontaneous which occurs without lung disease usually in young males, secondary spontaneous which occurs with underlying lung pathology, or traumatic. Types include closed which seals off, open with a bronchopleural fistula, and tension which increases pressure. Clinical features include chest pain and shortness of breath. Diagnosis is made with chest x-ray showing increased radiolucency. Small primary pneumothoraces may resolve on their own while secondary pneumothoraces and those with symptoms require tube thoracostomy drainage. Recurrent cases require pleurodesis or surgery.










































































