Downloaded 919 times









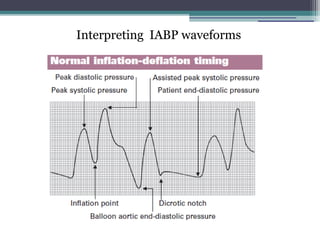
























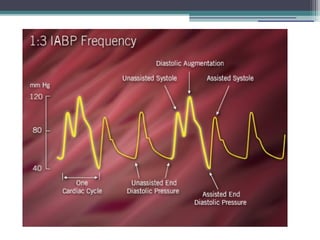





















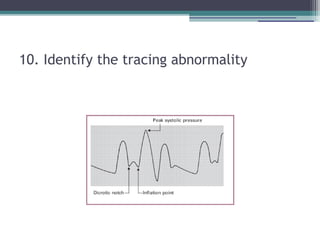









1) Intra-aortic balloon counterpulsation (IABP) provides systolic unloading and diastolic augmentation to improve cardiac output. 2) IABP is indicated for cardiogenic shock, high-risk PCI/CABG, and mechanical complications. 3) Potential complications include limb ischemia, infection, bleeding, and aortic injury. 4) Optimal IABP waveform analysis and timing are important to maximize hemodynamic support.













































![INTRA AORTIC BALLON PUMP [IABP].ppt news](https://cdn.slidesharecdn.com/ss_thumbnails/intraaorticballonpumpiabp-240723151642-9cbe1595-thumbnail.jpg?width=640&height=640&fit=bounds)









































