Downloaded 291 times
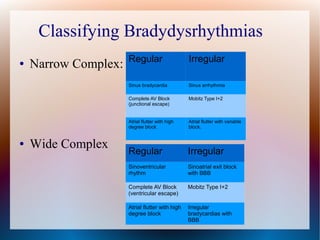
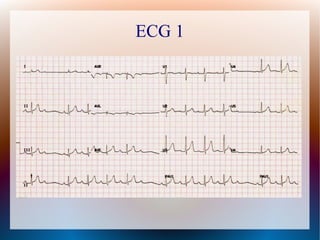
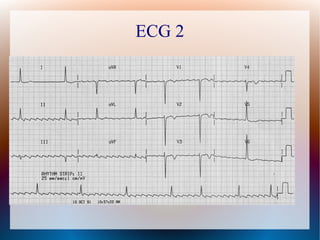

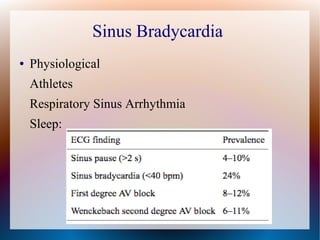
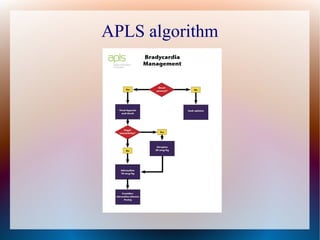
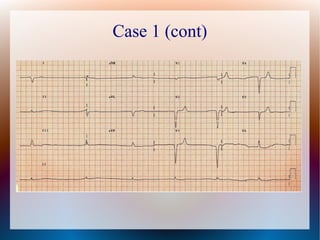
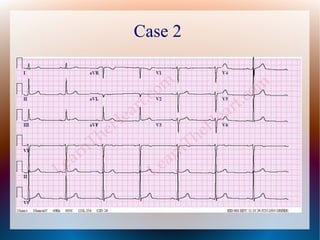

This document discusses the classification, causes, symptoms, and treatment of bradycardia. It defines different types of bradycardia based on rhythm and heart block. Common causes include medications, cardiac disease, metabolic abnormalities, and neurological or infectious etiologies. Symptoms range from dizziness to hypotension and shock. Treatment follows ACLS algorithms and may include atropine, transcutaneous pacing, or addressing underlying causes. Case examples demonstrate ECG findings and management of hyperkalemia-induced complete heart block, athlete's heart, and inferior STEMI with complete heart block.























































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)