Downloaded 278 times
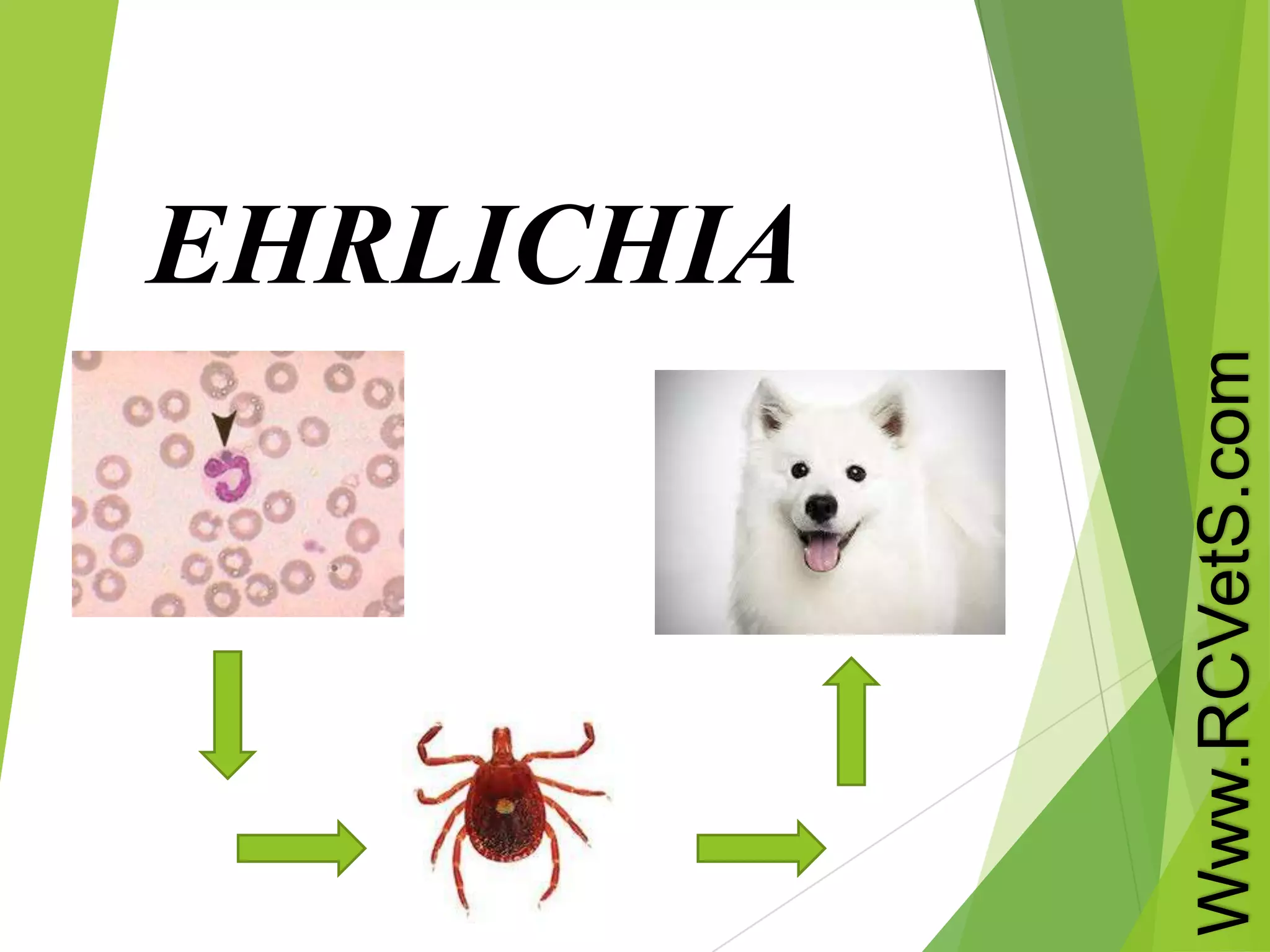
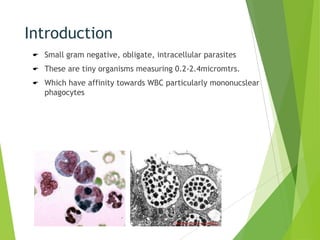
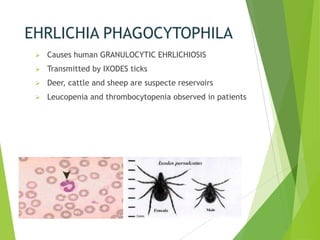

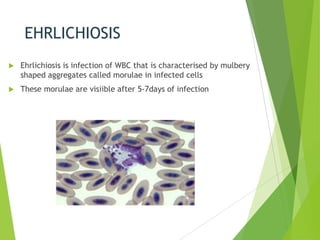
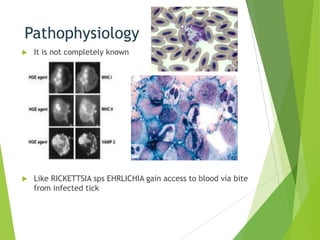
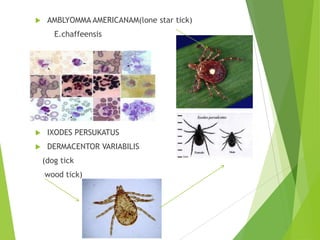
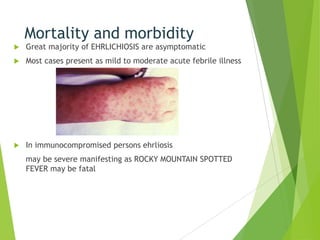


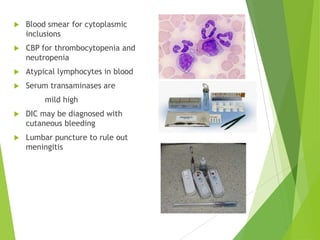



Ehrlichia are small, obligate intracellular parasites that infect white blood cells, particularly monocytes. They form clusters called morulae within the host cell. Ehrlichia species include E. sennetsu, E. caffeensis, E. phagocytophila, and E. canis. E. sennetsu causes glandular fever in Asia through fish consumption. E. phagocytophila causes human granulocytic ehrlichiosis through Ixodes ticks. E. caffeensis causes human monocytic ehrlichiosis through Amblyomma ticks. Ehrlichiosis is characterized by morulae in infected cells after 5-7 days. Most cases present as a mild acute fever but











































































































