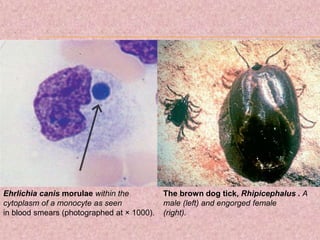
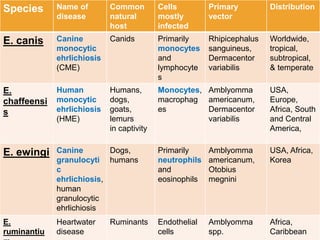
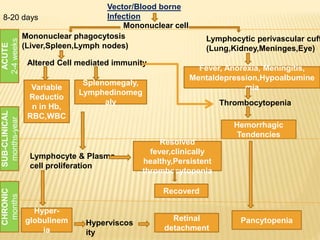
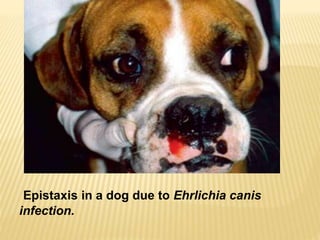
Dr. Ram Chander Tiwari presented a seminar on Canine Monocytotropic Ehrlichiosis. The disease is caused by Ehrlichia canis bacteria and transmitted by the brown dog tick Rhipicephalus sanguineus. Clinical signs include fever, lethargy, anemia, and hemorrhaging. Diagnosis involves detecting antibodies, observing morulae in blood smears, or PCR testing. Treatment involves doxycycline or tetracycline antibiotics for 3-4 weeks along with supportive care. Prevention focuses on tick control and testing dogs before introduction to kennels.