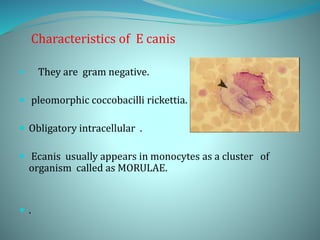
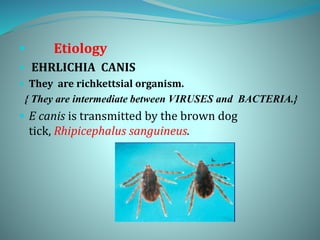
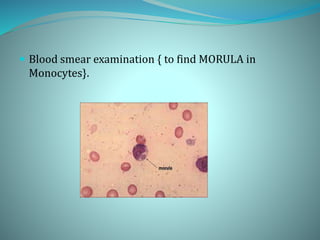
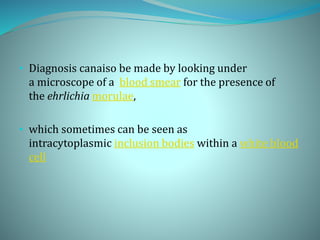
Ehrlichiosis is a tick-borne disease caused by Ehrlichia canis, a rickettsial organism. E. canis infects monocytes and forms clusters called morulae. It is transmitted by the brown dog tick Rhipicephalus sanguineus. Clinical signs include fever, lethargy, anorexia, thrombocytopenia, and hemorrhaging. Diagnosis involves identifying morulae in blood smears, serology tests, or PCR. Treatment is doxycycline for 3-4 weeks. Prevention focuses on tick control and chemoprophylaxis with tetracyclines.