
Downloaded 3,067 times
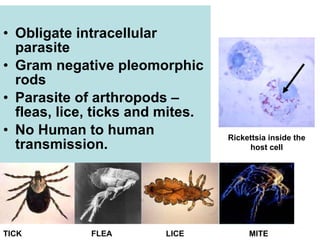
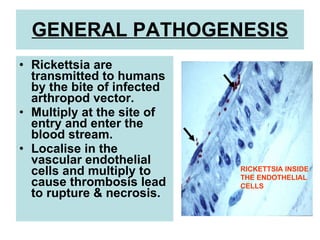

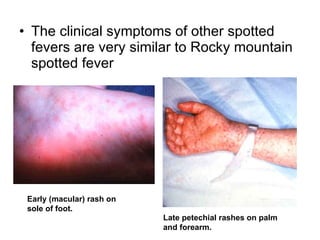
This document summarizes rickettsial diseases, which are caused by obligate intracellular parasites called Rickettsia. Rickettsia species are transmitted to humans via the bites of infected arthropods like fleas, lice, ticks and mites. Some key Rickettsia species and the diseases they cause include R. prowazekii which causes epidemic typhus, R. typhi which causes endemic typhus, and R. rickettsii which causes Rocky Mountain spotted fever. Symptoms include fever, headache, rash and potentially serious complications if left untreated. Diagnosis involves isolation of the bacteria or serological tests to detect antibodies. Treatment is with doxycycline or tetracycline.



















































































