

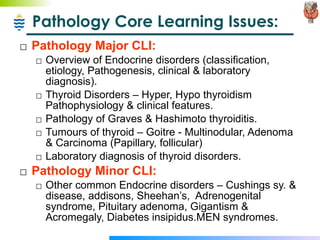
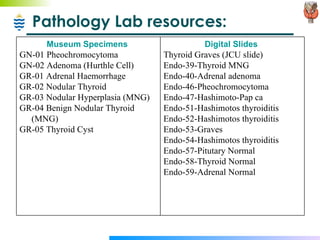
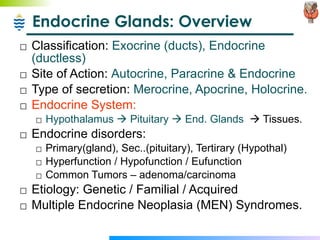

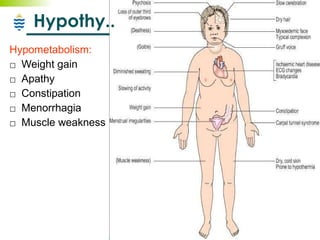
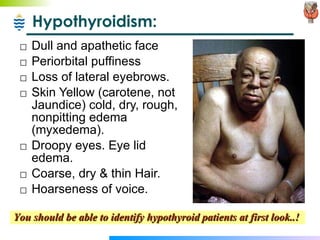
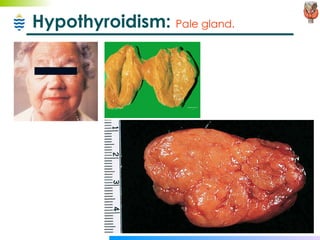
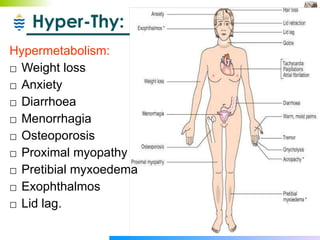
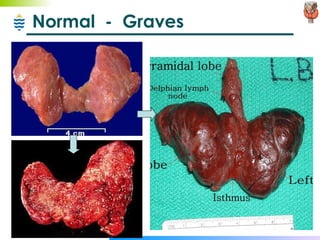
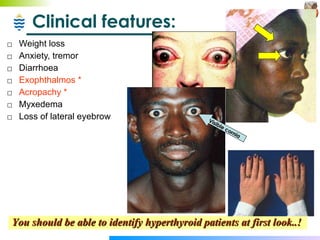
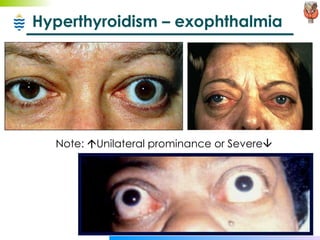
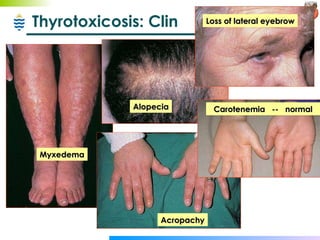
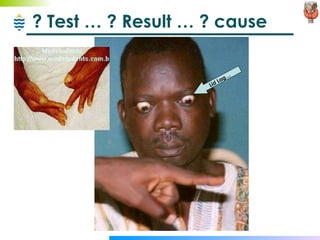
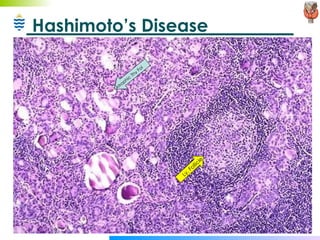
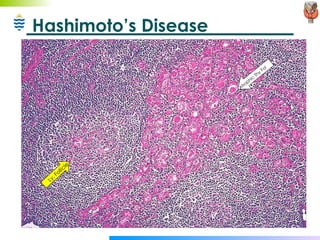
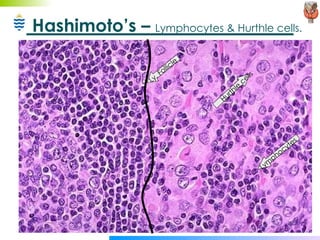
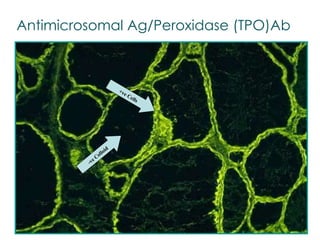

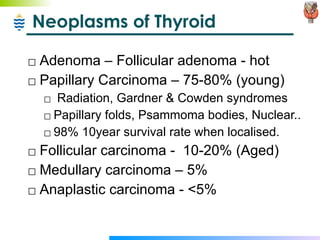
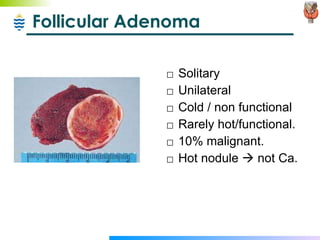
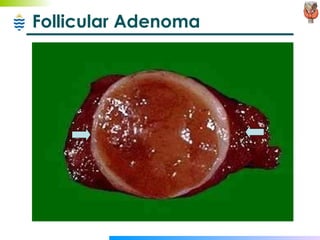

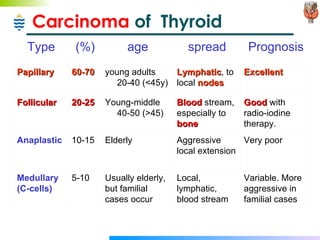

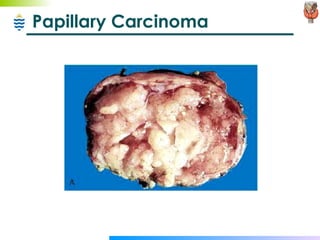
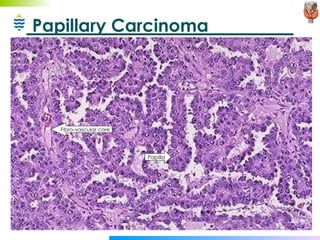
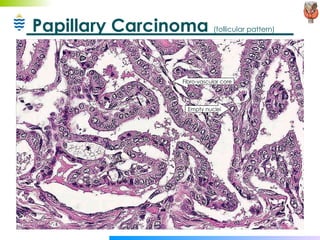
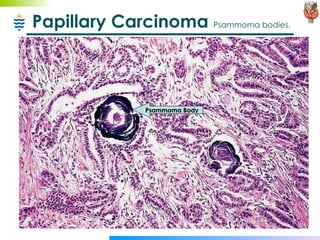
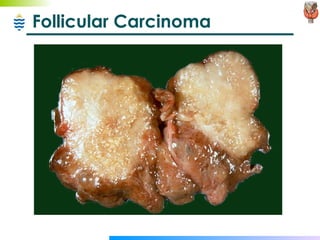
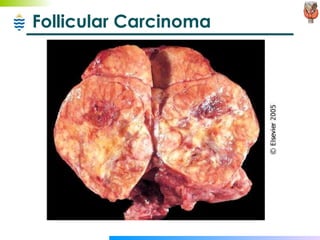
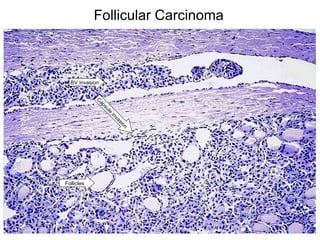
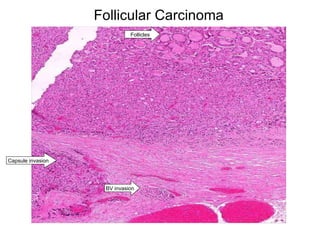
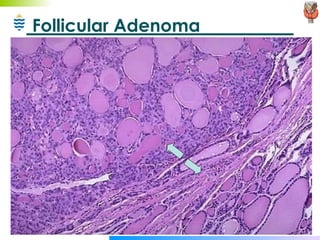
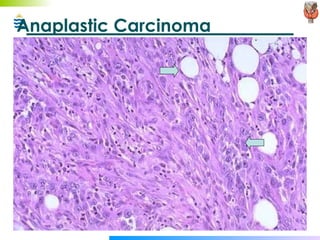
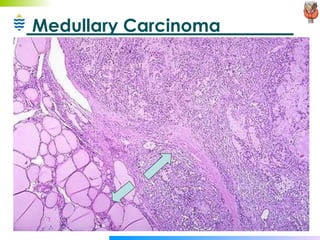



The document discusses thyroid pathology including: - Types of thyroid disorders - hyperthyroidism, hypothyroidism, and euthyroid goiters. - Common causes like Graves' disease, Hashimoto's thyroiditis, multinodular goiter. - Clinical features of hyperthyroidism and hypothyroidism. - Investigations like thyroid function tests and radioactive iodine uptake scans. - Microscopic findings in various thyroid conditions. - Thyroid neoplasms including adenomas, papillary carcinoma, follicular carcinoma, and others.
































































![Thyroid pathophysiology scintigraphy[1]](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidpathophysiologyscintigraphy1-161007125709-thumbnail.jpg?width=640&height=640&fit=bounds)

































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







