Downloaded 367 times

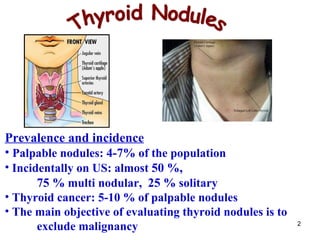
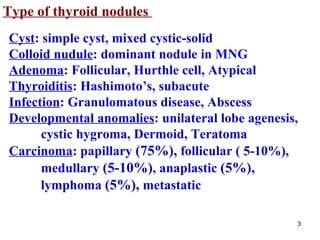
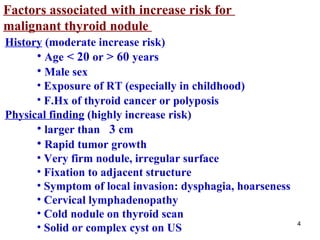
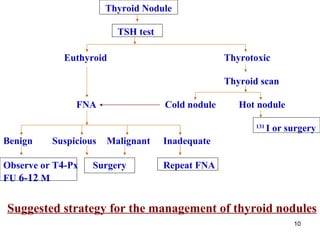
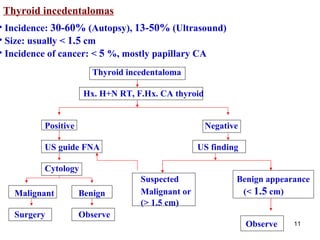
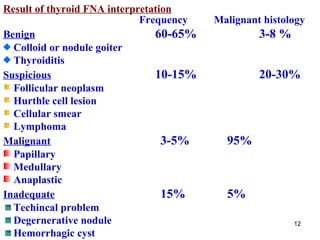

- Thyroid nodules are very common, found in 4-7% of people on physical exam and almost 50% on ultrasound, with most people having multiple nodules. Thyroid cancer is found in 5-10% of palpable nodules. - Factors that increase cancer risk include nodule size over 3 cm, male sex, radiation exposure, family history of thyroid cancer, and symptoms of local invasion. Features suggesting benign nodules include a family history of autoimmune disease and benign nodules. - Evaluation involves ultrasound, thyroid function tests, and fine needle aspiration of suspicious nodules, with surgery for nodules found to be malignant or indeterminate




























































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)







