INTRODUCTION
• Thyroid gland: endocrine gland .
• In 1776, Albert von haller classified thyroid as ductless gland.
• 1st thyroid sx—for t/t of goitre by Roger frugardi in1170.
EMBRYOLOGY
• It arises as outpouching of primitive foregut at 3rd wk gestation, originates at base
of tongue at foramen cecum and descent downward.
during descent remains connected to foramen cecum via thyroglossal duct.
medial thyroid anlage →thyroid follicle cells→appear by 8th wk IUL ,Colloid
formation begin by 11th wk IUL
lateral thyroid anlage→fuses with medial at 5th wk IUL
→ originate from 4th branchial arch→parafollicular
cells.
Thyroglossal duct→starts obliterating by 5th wk IUL, Disappears by 8th wk IUL.
3.
ANATOMY
• WT= 20-25GM
• C5-T1, Isthmus at C7
• enveloped by a fascia formed from partition of deep cervical fascia into
anterior and posterior division.
• True capsule: pereipheral condensation of fibrous stroma. is densly adherent
fibrous layer that sends out septa that invaginates into the gland forming
pseudolobule.
• capsule is condensed into berry ligament near cricoid cartilage.
• Blood supply: superior thyrod artery ← ECA
inferior thyroid artery← Thyrocervical trunk
Thyroid ima (in 1-4%)←aorta
venous drainage: superior thyroid vein→ IJV
middle thyroid vein → IJV
inferior thyroid vein→Brachiocephalic vein
SIMPLE GOITER
• enlargementof thyroid gland, may be difffuse, uninodular or multinodular
• d/t stimulation of thyroid gland by TSH
• Elevated TSH levels induce diffuse thyroid hyperplasia, followed by focal hyperplasia, resulting
in nodules that may or may not concentrate iodine, colloid nodules, or microfollicular nodules.
• Initially Persistent growth stimulation – diffuse hyperplasia
• Later Fluctuating stimulation – mixed pattern with areas of active lobules and inactive lobules
• Active lobules – become more vascular & hyperplastic – hemorrhage occurs– central necrosis
• Necrotic lobules coalesce – nodules filled with iodine free colloid or mass of new but inactive
follicles
• Continual repetition of process – results in nodular goitre
• Etiology: Puberty, pregnancy, familial,endemic, Dyshormonogenesis, goitrogens
• C/F: Mostly asymptomatic
compression symptoms- dysphagia, dyspnea
pemberton sign - d/t impaired venous return at thoracic inlet, mainly with substernal
goiter
acute pain - d/t sudden enlargement of nodule d/t hemorrhage
6.
DIFFUSE HYPERPLASTIC GOITER
•Corresponds to first stage of natural history
• d/t persistent TSH stimulation, diffuse
hyperplasia of gland
• Goitre in childhood usually seen in endemic
areas,
sporadic cases usually occurs in puberty
• Goitre is soft, diffuse, large enough to cause
discomfort
• Colloid goitre occurs in late stage when TSH
stimulation has fallen off
7.
MULTINODULAR GOITER
• h/olong standing goiter may be
present
• thyroid nodules become autonomus
over several years causing
hyperthyroidism.
• C/P - Females-late 30s or 40s-multiple
palpable nodules
• Occasionally a solitary nodule may be
palpable but there are multiple small
nodules impalpable.
• Nodules may be colloid or cellular,
cystic degeneration and hemorrhage
are common
8.
.• c/f: Hyperthyroidism:heat intolerance
thirst, increased sweting
wt loss
Dx: TFT: suppressed tsh level
USG: multiple nodules
RAI: hot and cold nodules
COMPLICATIONS: Secondary thyrotoxicosis – in about 30% nodular goitre.
:Tracheal obstruction – huge goitres or substernal prolongation of goitre
:Carcinoma (usually follicular)
T/T: Most patients are asymptomatic and do not need operation
Operation may be indicated on cosmetic grounds, for pressure symptoms, or in
response to patient anxiety
Choice of surgery
• Total thyroidectomy
• Subtotal thyroidectomy
• Total lobectomy
9.
THYROID CYST
• >30%of clinically isolated swellings contain fluid-are cystic or
partially cystic.
• Tense cysts – hard &mimic carcinoma
• Bleeding into cysts- acute painful swelling.
• 50% as a result of colloid degeneration or of uncertain etiology like
absence of epithelial cells in the lining.
• 10–15 per cent of cystic follicular swellings are histologically
malignant (30 per cent in men and 10 per cent in women).
• Papillary carcinoma is often associated with cyst formation
• C/P- In women aged 20-40 yrs - as discrete swellings
• Appropriate investigation : FNAC
10.
HASHIMOTO THYROIDITIS
• Autoimmunedisease. Ab against tpo,tsh receptor, tg
• Raised titres of thyroid antibodies.
• C/P : diffuse or nodular with a characteristic bosselated feel or subclinical thyroid
failure.
• painless anterior neck mass
• Onset may be insidious and asymptomatic or sudden and painful.
• Initially mild hyperthyroidism later hypothyroidism
• Goitre is usually lobulated ; diffuse or localised to one lobe.
• Large or small ; soft , rubbery or firm in consistency- depending on cellularity and
degree of fibrosis.
• gland infiltrated by lymphoid and plasma cells, follicles lined by hurthle cell
characterized by abundant eosinophilic cytoplasm
• Mc –women 30-50 yr ,M:F= 1:10 To1:20
• DIAGNOSIS- Raised serum levels of thyroid antibodies + raised TSH, FNAC, diagnostic
lobectomy
• T/T: Hr replacement to maintain TSH( For TSH >10IU/ml OR Ab +ve)
11.
DE QUERVEIN THYROIDITIS
•Granulomatous thyroiditis, subacute thyroiditis
• May follow viral infection
• C/F: pain in neck , fever , malaise and firm, irregular enlargement of one
or both thyroid lobes
• Raised inflammatory markers , absent thyroid antibodies , serum T4 is
slightly raised
• Self limiting - a period of months of hypothyroidism may be present
before eventual recovery
• DIAGNOSIS - FNAC , radioactive iodine uptake and by rapid symptomatic
response to prednisolone.
• TREATMENT- PREDNISOLONE 10-20mg daily for 1 week & then gradually
reduced dose over next month
12.
RIEDEL THYROIDITIS
• Veryrare - 0.5% of goitres.
• Thyroid tissue replaced by cellular fibrous tissue - infiltrates through capsule
into muscle and adjacent structures including parathyroid, recurrent nerves,
carotid sheath.
• Probably a collagen disease
• Predominantly in women 30-60yr
• painless, hard, anterior neck mass
• Goitre may be U/L or B/L - very hard and fixed. HARD WOODY THYROID
• compression s/s: dysphagia, dyspnea, choking, hoarseness
• TREATMENT-High dose steroid, tamoxifen, thyroxine replacement
13.
ACUTE BACTERIAL THYROIDITIS
•M/c in children, preceeded by URTI or otitis media
• c/f : severe neck pain radiating to jaw ,fever ,chills,dysphonia,
odynophagia
• complication: systemic sepsis, juglar vein thrombosis, tracheal or
esophageal rupture.
• dx: fnab, leucocytosis
• t/t: antibiotics, abscess drainage
EYE SIGNS
LID RETRACTION
•Over activity of involuntary part of the levator palpebrae superioris muscle.
• The upper eye lid is higher than normal and the lower eyelid is in its normal position
Exophthalmos
• eyeball is pushed forwards due to increase in fat or oedema or cellular infiltration in the retro orbital
space ,the eyelids are retracted and sclera becomes visible below the lower edge of the iris first
followed by above the upper edge of the iris.
• Von Graefe's sign.— The upper eyelid lags behind the eyeball as the patient is asked to look
downwards.
• Stellwag's sign — This is staring look and infrequent blinking of eyes with widening of palpebral fissure
• Joffroy’s sign – absence of wrinkling on forehead when patient looks up with head bent down.
• Moebius' sign — Inability or failure to converge the eyeballs.
• Dalrymple's sign— The upper sclera is visible due to retraction of upper eye lid
• Ophthalmoplegia
• Chemosis, papilloedema, corneal ulcer
16.
.
Ix:TFT- Increased T3T4, decreased TSH
• Radioisotope study – I123
more uptake – hot nodules
• TRH estimation
• ECG- cardiac involvement
• Thyroid antibody estimation
T/t:Antithyroid drugs
• Methimazole 20 – 40 mg OD (blocks thyroid hormone synthesis)
• Carbimazole 5-10 mg three times a day
• Propyl thiouracil 200 mg three times a day (blocks thyroid hormone
synthesis as well as blocks peripheral conversion of T4 to T3)
• Iodides – reduce vascularity
• Steroids
:Radioactive iodine therapy – I131
• Destroys cells and cause complete ablation of thyroid gland
• Usual dose- 5 to 10 millicurie or 160 microcurie/gm of thyroid
17.
.
Surgery
• Total thyroidectomy
•Subtotal thyroidectomy
• Hemithyroidectomy
SYMPTOMATIC T/t
• Beta blocker- control cardiovascular manifestation
• Calcium channel blocker
18.
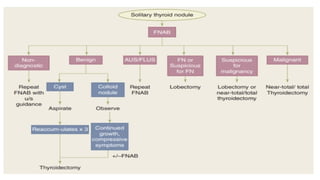
SOLITARY THYROID NODULE
•Single nodule palpable, rest gland not palpable.
• Cause: thyroid adenoma, carcinoma, cyst, thyroiditis
• usually painless
• a/w low dose ionizing radiation exposure
• risk factor for ca thyroid
• Dx: FNAB
• Ix: usg: differentiate solid from cystic, benign from neoplastic; fine
stippled calcification in neoplastic



![Dr.Ashish Mishra Seminar Thyroid disorders [Autosaved].pdf](https://cdn.slidesharecdn.com/ss_thumbnails/dr-230822194745-383295a9-thumbnail.jpg?width=640&height=640&fit=bounds)







![THYROID_GLAND[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/thyroidgland1-231005071359-bdb08841-thumbnail.jpg?width=640&height=640&fit=bounds)




































