Download as PDF, PPTX
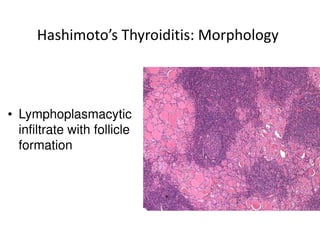
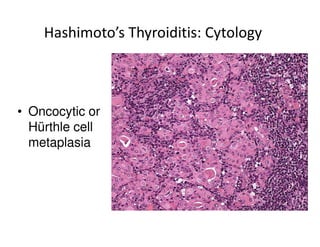
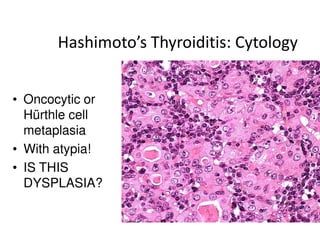
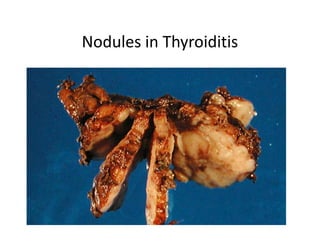
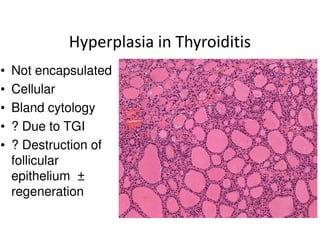
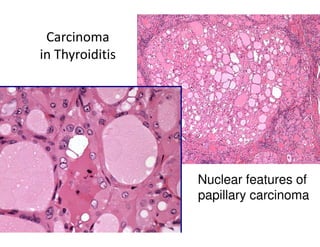
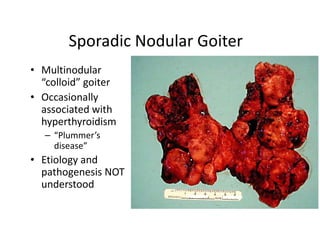
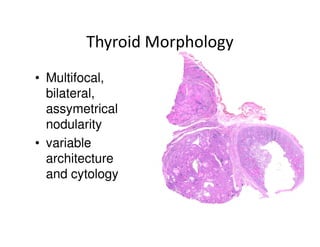
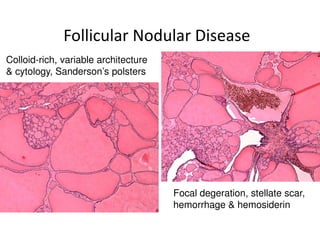
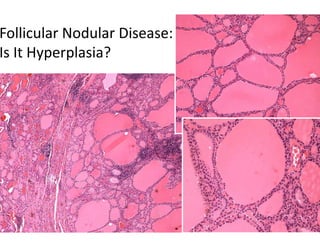
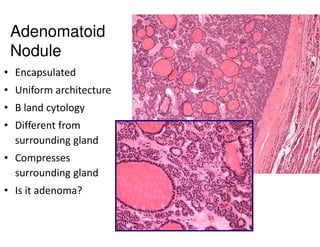
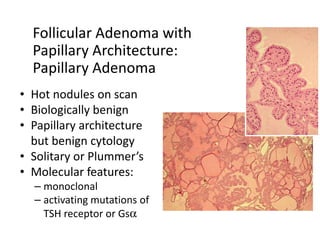
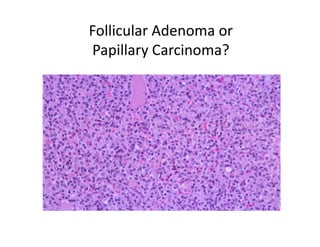
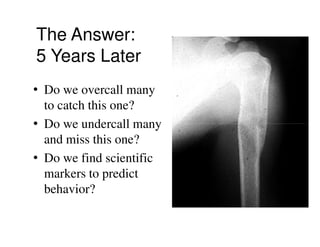
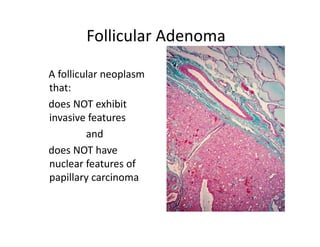
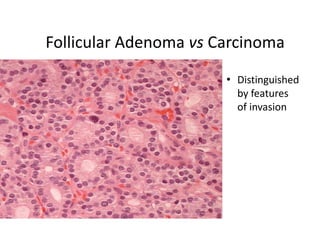
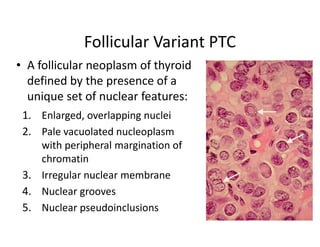

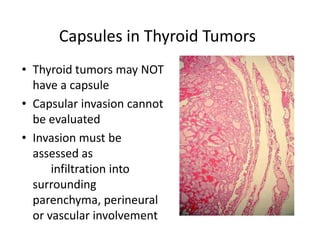
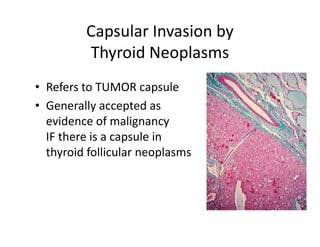
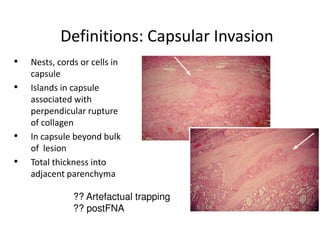
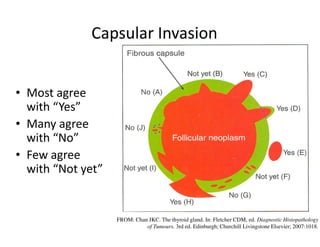
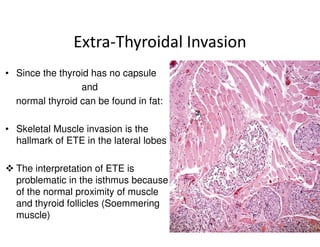
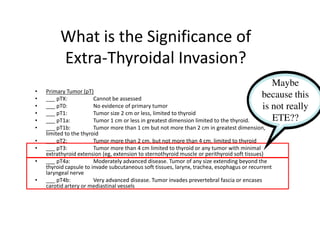
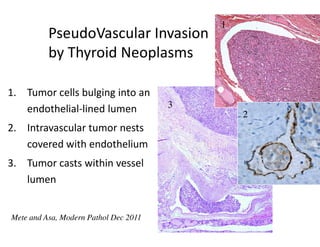
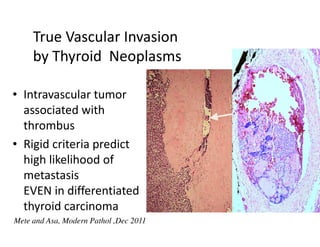

This document discusses several areas of controversy in thyroid pathology. It begins by outlining controversies regarding nodules found in thyroiditis, sporadic nodular goiter, papillary adenomas, follicular variant papillary carcinoma versus follicular carcinoma, capsular invasion, extrathyroidal extension, and vascular invasion. For each topic, the document provides histological images and discusses challenges in distinguishing hyperplasia from neoplasia, defining diagnostic criteria, and predicting tumor behavior. It emphasizes the need for further scientific study to help resolve some of these controversial gray zones in thyroid pathology.