Downloaded 203 times

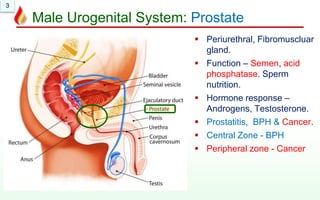
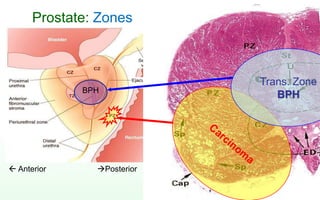
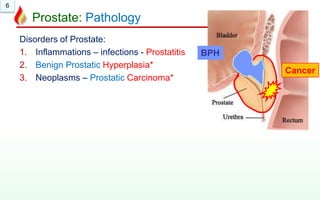
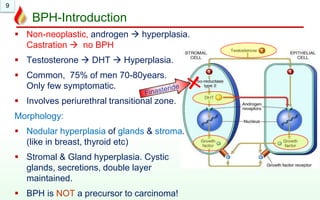
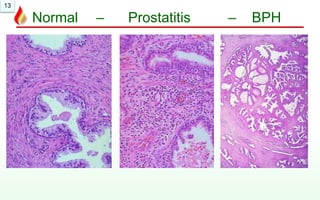

This document discusses benign prostatic hyperplasia (BPH): 1. BPH is a non-cancerous enlargement of the prostate gland caused by testosterone-driven hyperplasia. It commonly affects men over 70 years old. 2. Microscopically, BPH shows nodular hyperplasia of prostate glands and stroma, with cystic glands and retained double epithelial layer. 3. Clinical complications can include urinary obstruction, retention, infections, and kidney damage if left untreated. Treatment may involve transurethral resection of the prostate (TURP).
































































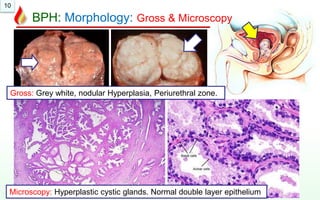
![Pathology_of_the_Prostate[1].pptx and prostate ca](https://cdn.slidesharecdn.com/ss_thumbnails/pathologyoftheprostate1-241210140819-e615f78e-thumbnail.jpg?width=640&height=640&fit=bounds)









































