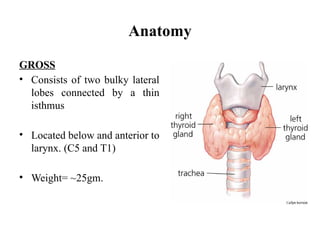
Anatomy
GROSS
• Consists oftwo bulky lateral
lobes connected by a thin
isthmus
• Located below and anterior to
larynx. (C5 and T1)
• Weight= ~25gm.
3.
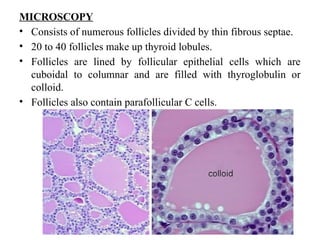
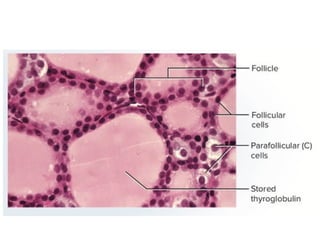
MICROSCOPY
• Consists ofnumerous follicles divided by thin fibrous septae.
• 20 to 40 follicles make up thyroid lobules.
• Follicles are lined by follicular epithelial cells which are
cuboidal to columnar and are filled with thyroglobulin or
colloid.
• Follicles also contain parafollicular C cells.
5.
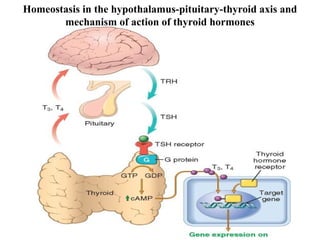
Homeostasis in thehypothalamus-pituitary-thyroid axis and
mechanism of action of thyroid hormones
6.
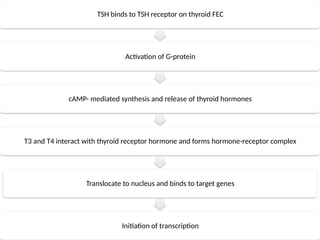
TSH binds toTSH receptor on thyroid FEC
Activation of G-protein
cAMP- mediated synthesis and release of thyroid hormones
T3 and T4 interact with thyroid receptor hormone and forms hormone-receptor complex
Translocate to nucleus and binds to target genes
Initiation of transcription
7.
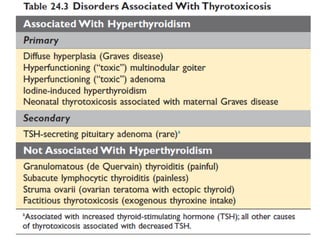
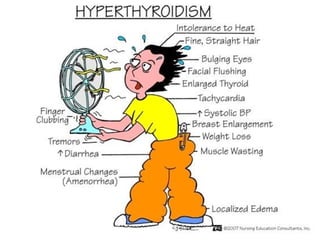
Hyperthyroidism
• Thyrotoxicosis isa hypermetabolic state caused by elevated
circulating levels of free T3 and T4.
• The three most common causes of thyrotoxicosis associated
with hyperfunction of the gland and include the following:
1. Diffuse hyperplasia of the thyroid associated with Graves
disease (accounts for 85% of cases)
2. Hyperfunctional multinodular goiter
3. Hyperfunctional adenoma of the thyroid
9.
Clinical features:
• Includeschanges referable to the hypermetabolic state induced by
excess thyroid hormone and to overactivity of the sympathetic
nervous system.
• Excess thyroid hormone increase in basal metabolic rate
resulting in:
– Soft, warm and flushed skin because of increased blood flow
and peripheral vasodilatation
– Increased sweating because of higher level of calorigenesis
– Weight loss due to heightened catabolic metabolism despite
increased appetite
11.
• Cardiac Manifestations:
–Elevated cardiac contractility and output in response to
increased peripheral oxygen requirement
– Tachycardia
– Palpitations
– Cardiomegaly
– Arrythmias such as atrial fibrillation
– Congestive heart failure
– Myocardial changes:
Focal lymphocytic and eosinophilic infiltrate
Mild fibrosis
Myofibril fatty change
Increase in size and number of mitochondria
12.
• Overactivity ofsympathetic nervous system produces:
– Tremor
– Hyperactivity
– Emotional lability
– Anxiety
– Inability to concentrate
– Insomnia
– Proximal muscle weakness and decreased muscle mass
(thyroid myopathy)
– In GI hyperdefecation due to hypermotility and reduced
transit times
13.
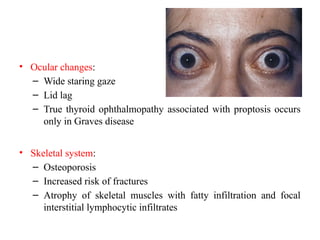
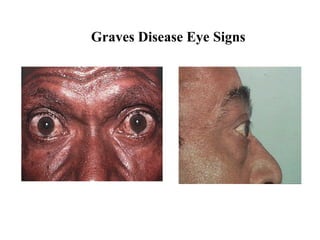
• Ocular changes:
–Wide staring gaze
– Lid lag
– True thyroid ophthalmopathy associated with proptosis occurs
only in Graves disease
• Skeletal system:
– Osteoporosis
– Increased risk of fractures
– Atrophy of skeletal muscles with fatty infiltration and focal
interstitial lymphocytic infiltrates
14.
• Mild hepatomegalydue to hepatic steatosis
• Generalised lymphoid hyperplasia
• Thyroid storm:
– Abrupt onset of severe hyperthyroidism
– It is a medical emergency
– Occurs most commonly in patient with Graves disease
– Results from acute elevation in catecholamines levels as
might be encountered during infection, surgery, cessation
of anti-thyroid medication or any form of stress
– Patient are often febrile and present with tachycardia
15.
Investigation
• TFTS:
Primary: <TSH,>T3 & T4
Secondary: Normal or > TSH,
• Radioiodide scan
• ELISA for anti –TSH receptor/TSI, antimicrosomal ab
• LFTS – elevated
• CBC- mild normocytic anemia, mild neutropenia, < Platelets
• Biopsy- FNA cytology
• USG
• CT/MRI – head/ chest
16.
Graves Disease
• Characterizedby a triad of clinical findings:
1.Hyperthyroidism due to diffuse, hyperfunctional enlargement of the
thyroid
2.Infiltrative ophthalmopathy with resultant exophthalmos
3.Localized, infiltrative dermopathy, sometimes called pretibial
myxedema, which is present in a minority of patients
• Peak incidence: 20 and 40 years of age
• Women are affected as much as 10 times more frequently than men.
• Patients are at increased risk for other autoimmune diseases, such
as systemic lupus erythematosus, pernicious anemia, type 1
diabetes, and Addison disease.
17.
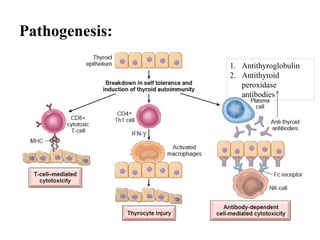
Pathogenesis:
• An autoimmunedisorder characterized by the production of
autoantibodies against multiple thyroid proteins, most
importantly the TSH receptor. Other: Thyroid peroxisomes
and Thyroglobulin.
• The most common antibody subtype, known as thyroid-
stimulating immunoglobulin (TSI), is observed in
approximately 90% of patients.
• Genetic susceptibility is associated with polymorphisms in
immune-function genes like CTLA4, PTPN22, and IL2RA.
18.
Clinical Features:
• Diffuseenlargement of the thyroid is present in all cases.
• Infiltrative ophthalmopathy is characteristic of Graves disease.
Activated
CD4+
helper T
cells
Secrete
cytokines
Stimulate
fibroblast
proliferation
and synthesis
of
extracellular
matrix
proteins
(glycosaminog
lycans),
Progressive
infiltration of
the retro-
orbital space
and
ophthalmopath
y
19.
• Protrusion ofthe eyeball (exopthalmos) is caused by an
increase in the volume of the retro-orbital connective tissues
and extraocular muscles, which occurs for several reasons:
i. Marked infiltration of connective tissue by mononuclear
cells, predominantly T cells
ii. Inflammation, edema, and swelling of extraocular
muscles
iii. Accumulation of extracellular matrix components,
specifically hydrophilic glycosaminoglycans such as
hyaluronic acid and chondroitin sulfate
iv. Increased numbers of adipocytes (fatty infiltration).
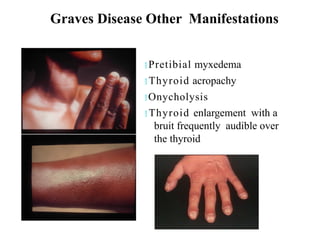
Graves Disease OtherManifestations
Pretibial myxedema
Thyroid acropachy
Onycholysis
Thyroid enlargement with a
bruit frequently audible over
the thyroid
22.
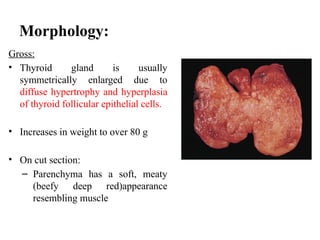
Morphology:
Gross:
• Thyroid glandis usually
symmetrically enlarged due to
diffuse hypertrophy and hyperplasia
of thyroid follicular epithelial cells.
• Increases in weight to over 80 g
• On cut section:
– Parenchyma has a soft, meaty
(beefy deep red)appearance
resembling muscle
23.
Microscopic:
• Follicle epithelialcells in untreated cases are tall and more crowded
than usual.
• Crowding often results in the formation of small papillae that project
into the follicle lumen and encroach on the colloid, sometimes filling
the follicles.
• Such papillae lack fibrovascular cores.
• Colloid within the follicle lumen is pale, with scalloped margins.
• Lymphoid infiltrates, consisting predominantly of T cells, along with
scattered B cells and mature plasma cells, are present throughout the
interstitium.
• Germinal centers are common.
• Changes inextrathyroidal tissue include:
i. Lymphoid hyperplasia, especially enlargement of the thymus
in younger patients.
ii. Heart may be hypertrophied, and ischemic changes may be
present.
iii. Dermopathy, if present, is characterized by thickening of the
dermis due to deposition of glycosaminoglycans and
lymphocyte infiltration.
26.
Laboratory findings:
• Elevatedfree T4 and T3 levels
• Depressed TSH levels
• Radioiodine scans show a diffusely increased uptake of iodine
in the thyroid gland.
27.
Hypothyroidism
• Fairly commondisorder
• Defn: A condition caused by a structural or functional derangement
that interferes with the production of thyroid hormone.
• Divided into primary and secondary categories, depending on whether
the hypothyroidism arises from an intrinsic abnormality in the thyroid
itself, or occurs as a result of pituitary and hypothalamic disease
• Primary hypothyroidism can be congenital, acquired, or autoimmune.
• Acquired hypothyroidism can be caused by surgical or radiation-
induced ablation of thyroid parenchyma, Drugs, hypopituitarism
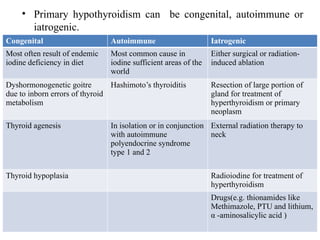
29.
• Primary hypothyroidismcan be congenital, autoimmune or
iatrogenic.
Congenital Autoimmune Iatrogenic
Most often result of endemic
iodine deficiency in diet
Most common cause in
iodine sufficient areas of the
world
Either surgical or radiation-
induced ablation
Dyshormonogenetic goitre
due to inborn errors of thyroid
metabolism
Hashimoto’s thyroiditis Resection of large portion of
gland for treatment of
hyperthyroidism or primary
neoplasm
Thyroid agenesis In isolation or in conjunction
with autoimmune
polyendocrine syndrome
type 1 and 2
External radiation therapy to
neck
Thyroid hypoplasia Radioiodine for treatment of
hyperthyroidism
Drugs(e.g. thionamides like
Methimazole, PTU and lithium,
α -aminosalicylic acid )
30.
• Secondary orcentral hypothyroidism is caused by:
i. Deficiency of TSH
ii. Deficiency of TRH- less common
iii. Any causes of hypopituitarism
iv. Hypothalamic damage
31.
Investigations:
•TFTs
– Primary: HighTSH & low T4
– Central (2˚ & 3˚): Low T4, TSH inappropriately normal
for the low T4, coexisting hormone def.
•Lipid profiles – Fasting cholesterol and triglycerides may be
raised
•Muscle enzymes (CPK) – elevated
•CBC- anaemia (normocytic normochromic)
•CXR- Effusions
•CT head- sellar/ suprasellar region.
33.
HASHIMOTO THYROIDITIS
• Defn:An autoimmune disease that results in destruction of
thyroid gland and gradual and progressive thyroid failure.
• Most common cause of hypothyroidism.
• Goiter and intense lymphocytic infiltration of the thyroid
(struma lymphomatosa).
• 45 and 65 years of age, common in women than in men. (10:1
to 20:1)
Clinical Features:
• Painlessenlargement of the thyroid, associated with
hypothyroidism, in a middle-aged woman.
• Symmetric and diffuse enlargement
• Increased risk for developing other autoimmune diseases,
– endocrine: type 1 diabetes, autoimmune adrenalitis
– non- endocrine: systemic lupus erythematosus, myasthenia
gravis and Sjögren syndrome.
37.
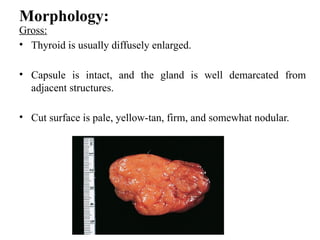
Morphology:
Gross:
• Thyroid isusually diffusely enlarged.
• Capsule is intact, and the gland is well demarcated from
adjacent structures.
• Cut surface is pale, yellow-tan, firm, and somewhat nodular.
38.
Microscopic:
• Extensive infiltrationof the parenchyma by a mononuclear
inflammatory infiltrate containing small lymphocytes, plasma
cells, and well-developed germinal centers.
• Thyroid follicles are atrophic and are lined in many areas by
epithelial cells with abundant eosinophilic, granular
cytoplasm, termed Hürthle cells.
• Interstitial connective tissue is increased and may be abundant.
39.
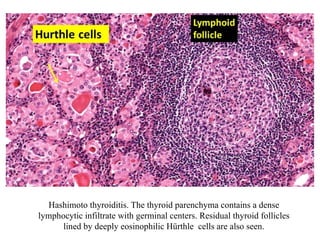
Hashimoto thyroiditis. Thethyroid parenchyma contains a dense
lymphocytic infiltrate with germinal centers. Residual thyroid follicles
lined by deeply eosinophilic Hürthle cells are also seen.