Downloaded 112 times
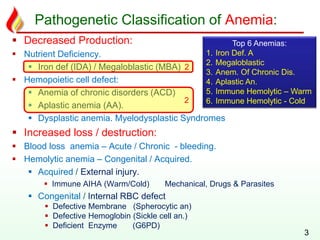
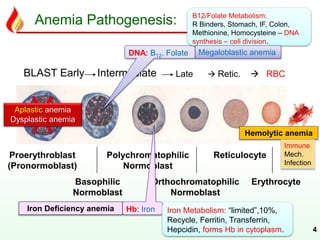
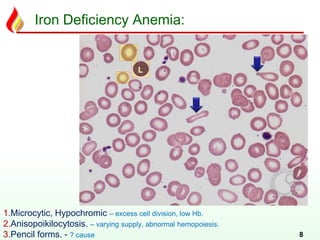


1. The document discusses various types of anemia classified by their pathogenesis into decreased red blood cell production, increased red blood cell destruction, and decreased red blood cell survival. 2. It provides details on the causes, pathogenesis, morphology, and clinical features of the most common anemias - iron deficiency anemia, megaloblastic anemia, anemia of chronic disease, aplastic anemia, and immune hemolytic anemia. 3. The learning objectives are to understand the overview, classification, pathogenesis, diagnosis, clinical features and complications of various anemias with a focus on studying the top 10 anemias in detail.






















































































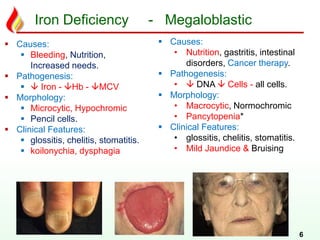
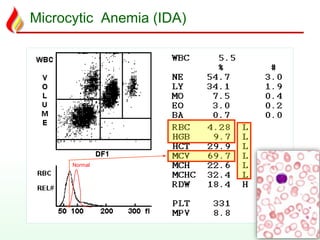
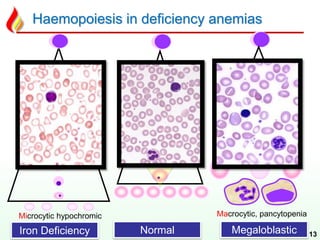
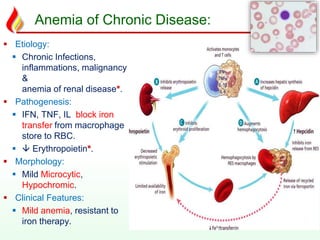
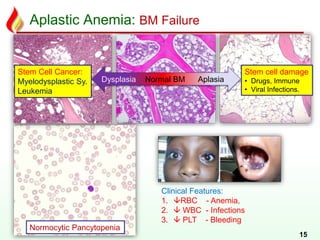
![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)









