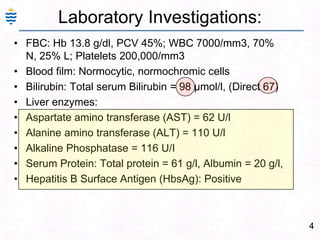
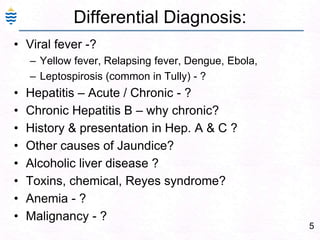




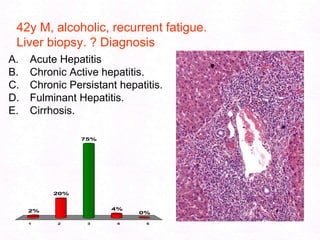

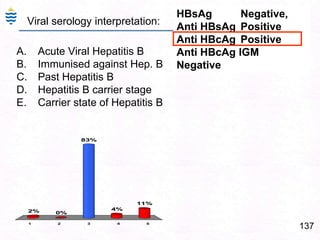
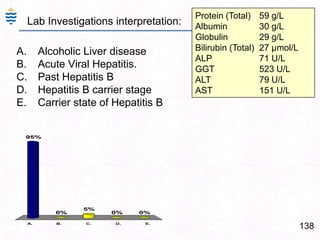
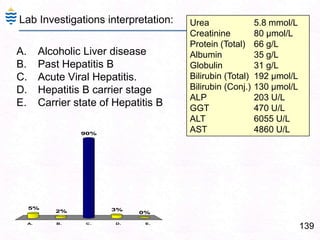
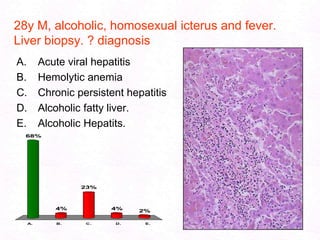
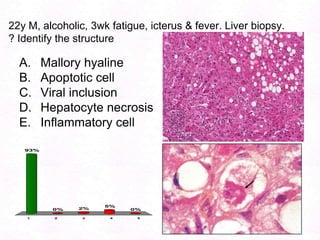
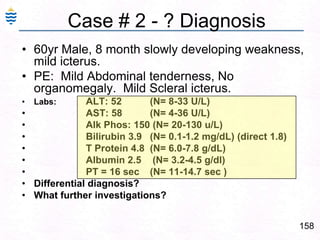

George, a 62-year-old farmer, presents with fatigue and yellowing of the eyes for 2 weeks. He reports weight loss but no other symptoms. Laboratory tests show elevated bilirubin and liver enzymes with positive hepatitis B surface antigen. The doctor considers diagnoses including acute or chronic hepatitis B, alcoholic liver disease, and other causes of jaundice. A liver biopsy may be needed to confirm chronic hepatitis B as the cause of the patient's chronic condition and symptoms.


















































![Acute and chronic liver disease [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/acuteandchronicliverdiseaseautosaved-250921172441-4babef2c-thumbnail.jpg?width=640&height=640&fit=bounds)





























![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)















