PRIMARY SURVEY
A:Able tospeak,No hoarseness,No C-spine tenderness
B:Normal chest expansion, clear and equal breath sound
both lungs
C:BP 117/77 mmHg,Pulse 84 rate /min,no active external
bleeding
D:E4V5M6 pupil 3 mm RTLBE
E:As shown on diagram
6.
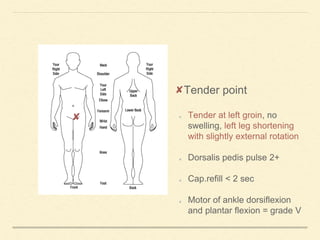
Tender point
Tender atleft groin, no
swelling, left leg shortening
with slightly external rotation
Dorsalis pedis pulse 2+
Cap.refill < 2 sec
Motor of ankle dorsiflexion
and plantar flexion = grade V
7.
Head and maxillofacial:
•No external wound,No facial deformity
C spine and neck:
• No wound at neck, active moment and full ROM
Chest
• Trachea in midline, no tender, no abrasion wound, no
subcutaneous emphysema, clear and equal breath sound both
lungs
PHYSICAL EXAMINATION
8.
Abdomen and Pelvis
Soft,nottender abdomen, tender at left groin area
Perineum and rectum
No ecchymosis
Musculoskeletal
Tender at left groin area, shortening of left extremity
Neurologic
GCS E4V5M6
Pupil 3 mm RTLBE,Full EOM
Motor: grade V except left lower extremity limit due to pain
PHYSICAL EXAMINATION
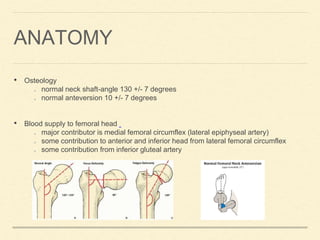
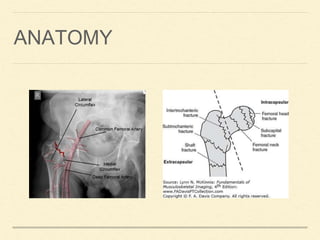
ANATOMY
• Osteology
normal neckshaft-angle 130 +/- 7 degrees
normal anteversion 10 +/- 7 degrees
• Blood supply to femoral head
major contributor is medial femoral circumflex (lateral epiphyseal artery)
some contribution to anterior and inferior head from lateral femoral circumflex
some contribution from inferior gluteal artery
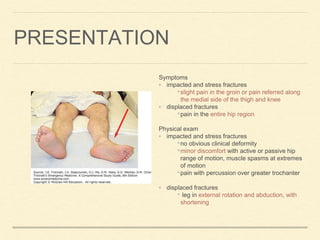
PRESENTATION
Symptoms
◦ impacted andstress fractures
•slight pain in the groin or pain referred along
the medial side of the thigh and knee
◦ displaced fractures
•pain in the entire hip region
Physical exam
◦ impacted and stress fractures
•no obvious clinical deformity
•minor discomfort with active or passive hip
range of motion, muscle spasms at extremes
of motion
•pain with percussion over greater trochanter
◦ displaced fractures
• leg in external rotation and abduction, with
shortening
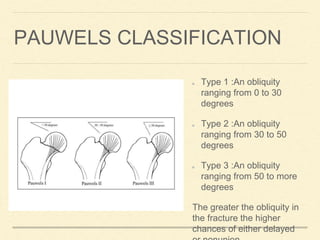
PAUWELS CLASSIFICATION
Type 1:An obliquity
ranging from 0 to 30
degrees
Type 2 :An obliquity
ranging from 30 to 50
degrees
Type 3 :An obliquity
ranging from 50 to more
degrees
The greater the obliquity in
the fracture the higher
chances of either delayed
18.
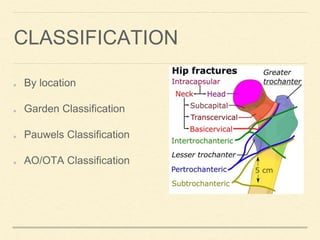
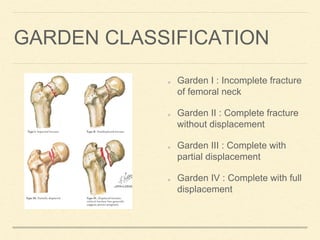
GARDEN CLASSIFICATION
Garden I: Incomplete fracture
of femoral neck
Garden II : Complete fracture
without displacement
Garden III : Complete with
partial displacement
Garden IV : Complete with full
displacement