Past History
■ ปฏิเสธโรคประจาตัว
■ปฏิเสธประวัติปวดหลังเป็นๆหายๆมาก่อนหน้า
■ ปฏิเสธประวัติการผ่าตัด
■ ปฏิเสธประวัติแพ้ยาแพ้อาหาร
■ ปฏิเสธประวัติสูบบุหรี่/ดื่มสุรา
5.
Physical Examination
■ Vitalsigns : BP 110/74 PR 68 RR 18 BT 36
■ General appearance : AThai muscular girl , Good
consciousness, not pale , no jaundice , anthalgic gait
■ HEENT : not pale conjunctivae , anicteric sclerae , no thyroid
gland enlargement , no cervical LN palpable
■ Cardiovascular : Full regular pulse both arms, no heaving , no
thrill ,normal S1S2 , no murmur
6.
Physical Examination
■ Respiratory: no chest wall deformities , no tachypnea ,
normal breath sounds both , no adventitious sound
■ Gastrointestinal : flat abdomen , normoactive bowel sound ,
soft not tender , no palpable mass , no hepatosplenomegaly ,
CVA not tender
■ Extremities : no deformities , no stiffness , full ROM both
hips,knees and ankles
7.
Physical Examination
■ Back: no scoliosis
■ tender with trigger point along paraspinous at upper
lumbar area
■ limit back flexion due to pain with sciatica
■ Trenderlenburg’s test + at Lt side
■ Straight leg rising test + Lt side at 45 degree
■ Lt lateral bending +
8.
Physical Examination
■ Neuro: Good consciousness , Alert ,Well orientation
■ CN : Intact all
■ Sensory : Grossly intact
■ Motor : normal muscle tone
■ Motor power RT LT
– Hip flex/extend V/V V/V
– Knee flex/extend V/V V/V
– Ankle flex/extend V/V V/V
– EHL V IV
■ BBK –
■ DTR 2+ all
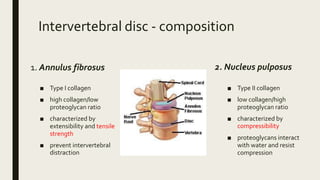
Intervertebral disc -composition
1. Annulus fibrosus
■ Type I collagen
■ high collagen/low
proteoglycan ratio
■ characterized by
extensibility and tensile
strength
■ prevent intervertebral
distraction
2. Nucleus pulposus
■ Type II collagen
■ low collagen/high
proteoglycan ratio
■ characterized by
compressibility
■ proteoglycans interact
with water and resist
compression
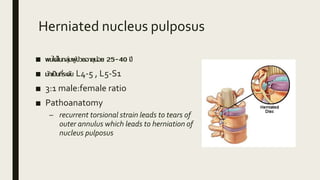
Herniated nucleus pulposus
■พบได้ในกลุ่มผู้ป่วยอายุน้อย 25-40 ปี
■ มักเป็นที่ระดับ L4-5 , L5-S1
■ 3:1 male:female ratio
■ Pathoanatomy
– recurrent torsional strain leads to tears of
outer annulus which leads to herniation of
nucleus pulposus
17.
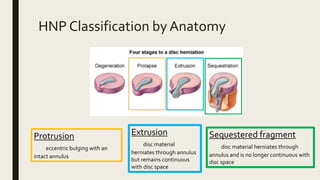
HNP Classification byAnatomy
Sequestered fragment
disc material herniates through
annulus and is no longer continuous with
disc space
Protrusion
eccentric bulging with an
intact annulus
Extrusion
disc material
herniates through annulus
but remains continuous
with disc space
18.
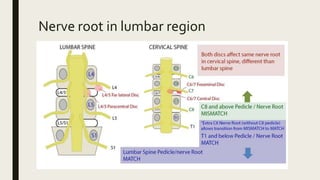
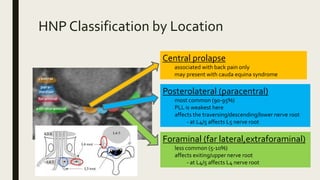
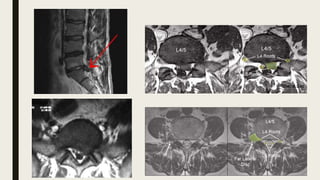
HNP Classification byLocation
Central prolapse
associated with back pain only
may present with cauda equina syndrome
Posterolateral (paracentral)
most common (90-95%)
PLL is weakest here
affects the traversing/descending/lower nerve root
- at L4/5 affects L5 nerve root
Foraminal (far lateral,extraforaminal)
less common (5-10%)
affects exiting/upper nerve root
- at L4/5 affects L4 nerve root
19.
Symptoms
“Sudden onset”
■ Axialback pain (low back pain)
■ Radicular pain (buttock and leg pain)
■ worsened by coughing, valsalva, sneezing , sitting
■ relieve when stay at supine position
■ Cauda equina syndrome (present in 1-10%)
■ bilateral leg pain
■ LE weakness
■ saddle anesthesia
■ bowel/bladder symptoms
20.
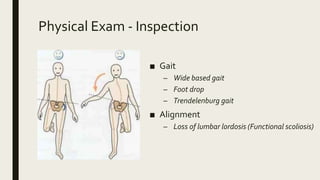
Physical Exam -Inspection
■ Gait
– Wide based gait
– Foot drop
– Trendelenburg gait
■ Alignment
– Loss of lumbar lordosis (Functional scoliosis)
21.
Physical Exam -Palpitation
■ Bone
■ Muscle
– Muscle spasm at the back ->
limit lumbar flexion
22.
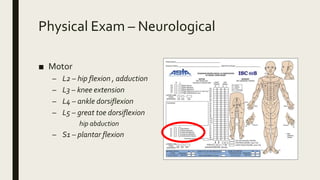
Physical Exam –Neurological
■ Motor
– L2 – hip flexion , adduction
– L3 – knee extension
– L4 – ankle dorsiflexion
– L5 – great toe dorsiflexion
hip abduction
– S1 – plantar flexion
23.
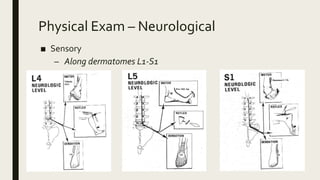
Physical Exam –Neurological
■ Sensory
– Along dermatomes L1-S1
24.
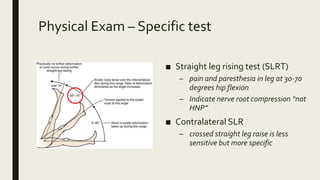
Physical Exam –Specific test
■ Straight leg rising test (SLRT)
– pain and paresthesia in leg at 30-70
degrees hip flexion
– Indicate nerve root compression “not
HNP”
■ Contralateral SLR
– crossed straight leg raise is less
sensitive but more specific
25.
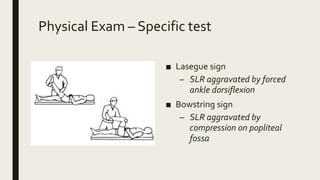
Physical Exam –Specific test
■ Lasegue sign
– SLR aggravated by forced
ankle dorsiflexion
■ Bowstring sign
– SLR aggravated by
compression on popliteal
fossa
26.
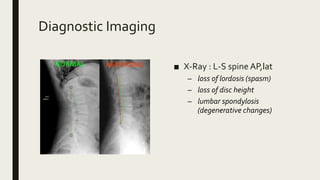
Diagnostic Imaging
■ X-Ray: L-S spine AP,lat
– loss of lordosis (spasm)
– loss of disc height
– lumbar spondylosis
(degenerative changes)
27.
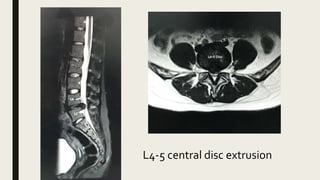
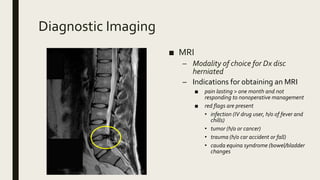
Diagnostic Imaging
■ MRI
–Modality of choice for Dx disc
herniated
– Indications for obtaining an MRI
■ pain lasting > one month and not
responding to nonoperative management
■ red flags are present
• infection (IV drug user, h/o of fever and
chills)
• tumor (h/o or cancer)
• trauma (h/o car accident or fall)
• cauda equina syndrome (bowel/bladder
changes