Primery Survey
A :can talk , not tender along C-spine , neck full ROM
B : spontaneous breathing , equal chest expansion , equal
breath sound , clear both lungs , CCT -
C : BP 96/58 mmHg , Heart rate 96/min , capillary refill <2
sec
D : E4V5M6 , pupil 3 mm RTLBE , motor grade V all
extremities , PR good sphincter tone
E : abrasion wound 3x4 cm at right knee , mild swelling ,
right leg deformity
4.
Secondary Survey
A :no history of drug or food allergy
M : no medication
P : no underlying disease
L : last meal at 18.00 ( 3 hrs PTA)
E : เกิดเหตุบนถนน ผู้ป่วยถูกรถกระบะชน กระเด็นเอาร่างกายด้านขวาลงกระแทก จาเหตุการณ์ได้
มีสติรู้ตัว แต่มีอาการมึนเมา หลังเกิดเหตุเจ็บหน้าอก คอ และปวดสะโพกขวามาก มีแผลที่เข่าขวา
5.
Physical Examination
GA :A middle age Thai man , good
consciousness , E4V5M6
HEENT : no discharge from eye or ear ,
no neck pain , no hematoma
Chest : equal chest movement , no stridor , clear and equal breath
sound , trachea in midline , equal tympanic on percussion
Heart : normal S1,S2 , no murmur , distal pulse can be palpated
Abdomen : soft , not tender , no guarding . no rebound tenderness
Neuro : pupil 3 mm RTLBE , motor grade V all ext. , sensory intact ,
reflex 2+ all , PR good sphincter tone
V/S : BP 96/58 mmHg BT 36.7 HR 96 /min
RR 22 /min
6.
Extremity : Rt.Leg external rotation deformity , Rt.leg shorter
than left leg , cannot lift leg , no tender point , pelvic compression
negative , no wound , no swelling
Rt. Knee abrasion wound size 3x4 cm , no deformity , full ROM
Rt. Ankle no wound , not tender , full ROM
Physical Examination
FAST : negative
Film- C-spine : Closed fracture at spinous
processC3-C4
- Both Hip AP and Hip lateral :
Closed fracture at intertrochanter of right
femur
Investigation
13.
Treatment
- On skeletaltraction right leg 2 kg
- On Philadelphia collar
- NPO
- 5% DN/2 1000 ml IV rate 80 ml/hr
- CBC , BUN , Cr , Electrolyte
- Chest X-ray
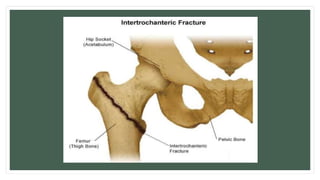
Definition
• An intertrochantericfracture occurs between the greater
and lesser trochanter, where the gluteus medius and
minimus muscle (hip extensor and abductor)attach, and the
lesser trochanter, where the iliopsoas muscle (hip
flexor)attaches.
17.
General Features
• Exuracapsularfracture with better healing potential
• Common in elderly osteoporotic patient, usually woman in
their 80’s
• More common than intracapsular
• Rarely causes avascular necrosis
18.
Mechanism of Injury
•In younger individual are usually the result of a high-energy
injury, such as a motor vehicle accident or fall from high.
• In elderly, it result from a simple fall.
19.
Signs and Symptoms
•Pain
• Marked shortening of lower limb
• Patient can not lift their leg
• Complete external rotation deformity
• Swelling, ecchymosis and tenderness over the greater trochanter
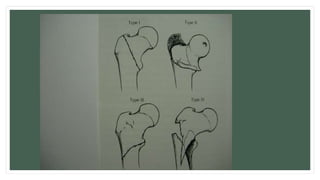
Classification(Boyd & Griffin)
Stablefractures
• Type I: Nondisplaced fracture
• Type II: Displaced fracture
Unstable fractures
• Type III: Reverse,subtrochanteric,or
posteromedial comminution fracture
• Type IV: Intertrochanteric fracture with
subtrochanteric fracture
23.
Stability of fracture
•Integrity of the posteromedial cortex is
the most important factor
• Reverse fracture is more unstable
• Subtrochanter fracture is more unstable
24.
Treament
- Nonoperative
nonweightbearing withearly out of bed to chair
indications
- nonambulatory patients
- patients at high risk for perioperative mortality
outcomes
- high rates of pneumonia, urinary tract infections, decubiti, and
DVT
25.
Treament
- Operative
- slidinghip compression screw
indications
- stable intertrochanteric fractures
- intramedullary hip screw (cephalomedullary nail)
indications
- stable fracture patterns
- unstable fracture patterns
- reverse obliquity fractures
56% failure when treated with sliding hip screw
- subtrochanteric extension
- lack of integrity of femoral wall
associated with increased displacement and collapse when treated with
sliding hip screw