Physical examination
• Vitalsigns: BP 121/72 mmHg PR 84 bpm
• T 36.8 c RR 20 bpm
• GA: a Thai teen-aged man, good consciousness, no
pallor, no jaundice, anthalgic gait
• HEENT : not pale conjunctivae, anicteric sclerae, no
thyroid gland enlargement ,no cervical LN palpable
• CVS : full regular symmetrical pulse all extremities
, normal S1 S2 no murmur
7.
• Lungs: normalbreath sound, equal both lung, no
adventitious sound
• Abdomen : soft, normoactive bowel sound, not
tender, no palpable mass, no hepatosplenomegaly
• Extremities : no deformities, no pitting edema
: left side antalgic gait,
: no Trenderlenburg gait
8.
• Back: lossof lumbar lordosis , no scoliosis
: no mark pain on percussion, no trigger point
: Limitation of flexion due to pain
: SLR test positive at 40 degree Rt, 30 degree
Lt
: Laseque’s test positive
9.
• Neuro :good consciousness , alert
• CN : intact all
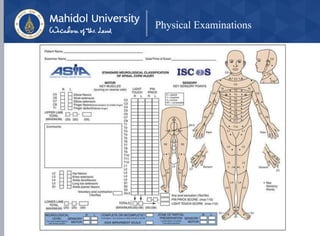
• Sensory : decrease sensation at Lt L3-L4-L5 S1-S2 ,
genitalia and perianal areas
• BBK – plantar flex both side
• DTR 2+ all
10.
Motor power RightLeft
• L2 hip flexors IV III
• L3 quadriceps V IV
• L4 tibialis anterior V III
• L5 EHL V IV
• S1 peroneus, gastrocnemius V IV
• PR: Anal sphicter -- Loose sphincter tone
Note: C5-T1 motor power grade V both side
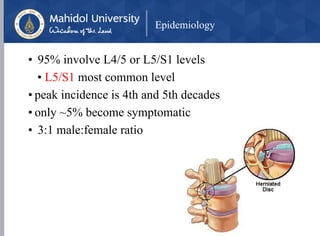
Epidemiology
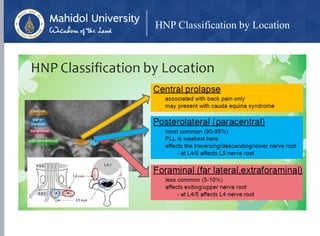
• 95% involveL4/5 or L5/S1 levels
• L5/S1 most common level
• peak incidence is 4th and 5th decades
• only ~5% become symptomatic
• 3:1 male:female ratio
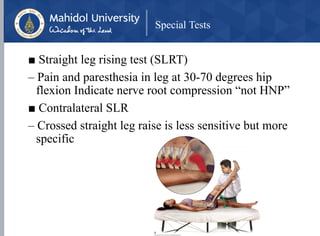
Special Tests
■ Straightleg rising test (SLRT)
– Pain and paresthesia in leg at 30-70 degrees hip
flexion Indicate nerve root compression “not HNP”
■ Contralateral SLR
– Crossed straight leg raise is less sensitive but more
specific
29.
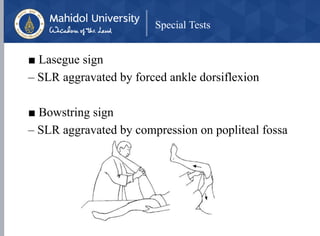
Special Tests
■ Laseguesign
– SLR aggravated by forced ankle dorsiflexion
■ Bowstring sign
– SLR aggravated by compression on popliteal fossa
30.
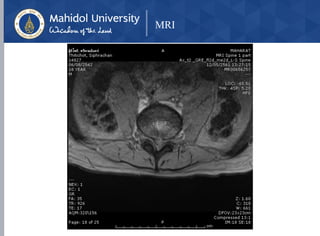
Diagnostic Imaging
• X-Ray: L-S spine AP, lateral
• loss of lordosis (spasm)
• loss of disc height
• lumbar spondylosis
• (deg
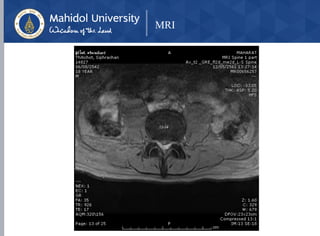
• MRI
• Modality of choice
• Indications for obtaining an MRI
• pain lasting > 1 month and not responding to
nonoperative management
• Red flags are presentenerative changes
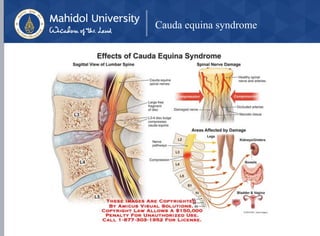
Cauda equina syndrome
•Cauda equina syndrome is defined by a constellation
of symptoms that result from terminal spinal nerve
root compression in the lumbosacral region
considered one of the few true medical emergencies
in orthopaedics
• key features
• bilateral leg pain
• bowel and bladder dysfunction
• saddle anesthesia
• lower extremity sensorimotor changes
36.
Cauda equina syndrome
•Epidemiology 1-6% of lumbar disc herniations
• Pathophysiology space-occupying lesion within
lumbosacral canal, including
• disc herniation (most common)
• spinal stenosis
• tumors
• trauma (retropulsion of fracture fragment, dislocation or
collapse)
• spinal epidural hematoma
• epidural abscess
37.
Cauda equina syndrome
•Operative urgent surgical decompression within
48 hours
• indications
• significant suspicion for CES
• severity of symptoms will increase the urgency of surgical
decompression
• techniques
• diskectomy
• laminectomy
• outcomes
• studies have shown improved outcomes in bowel and bladder
function and resolution of motor and sensory deficits when
decompression performed within 48 hours of the onset of
symptoms