PRIMARY SURVEY
• A– Can talk, no stridor, not tender along c-spine
• B – equal breath sound, RR 18/min, CCT neg
• C – BP 171/80 mmHg, PR 98 bpm
• D – E4V5M6, pupil 2mm RTLBE
• E – no wound at back, swelling and tender at left
knee with palpable bony stepping with limit ROM
due to pain
5.
SECONDARY SURVEY
• A– none
• M – amlodipine(5) 2x1 PO pc, simvastatin(10) 1
tab PO hs, MFM(300) 2x2 PO pc, Enalapril(5)
1x1PO pc, Glipizide(5) 2x2 PO ac, ASA(81) 1
tab PO hs
• P – HT, DM, DLP
• L – not known
• E – Fall from standing height
PHYSICAL EXAMINATION
• Vitalsigns – BT 36.8 C HR 98 /min
RR 18 /min BP 171/80 mmHg
• General appearance – good consciousness, not pale,
no jaundice, hyperstehenic built
• HEENT – not pale conjuctivae, anicteric sclerae
• Cardiovascular – pulse full and regular, normal s1&s2
sound, no murmur
• Lungs and chest – equal chest expansion, equal breath
sound
10.
PHYSICAL EXAMINATION
• Abdomen– soft, not tender, no distension
• Extremities – tender and swelling at left knee, loss of
extensor mechanism, neurovascular intact, DP/PT
pulse 2+, capillary refill <2 sec
• LN – no lymphadenopathy
• Neuro exam – E4V5M6 pupil 3 mm RTLBE
• Motor : grade V all extremities
• Sensation : intact
• DTR : 2+
FILM LEFT KNEEAP
• Patella in midline
• Seen transvers fracture line and
vertical line
• Distal pole higher than
tangential line < 20 mm
• No condylar or plateau fracture
• No bipartite patella
15.
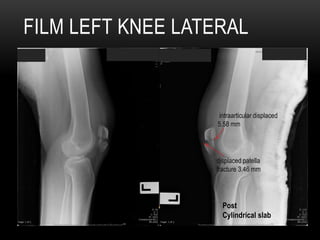
FILM LEFT KNEELATERAL
Post
Cylindrical slab
intraarticular displaced
5.58 mm
displaced patella
fracture 3.46 mm
16.
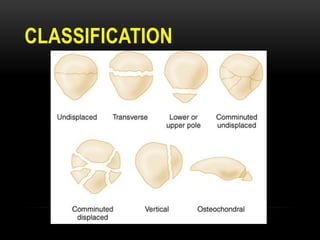
FINDINGS
• Closed completetransverse fracture of left patella
• Displaced patella fracture 3.46 mm (>3mm)
• Intraarticular displaced 5.58 mm (>2mm)
• Joint stepping
• Insall-Salvati ratio normal (height: patella/patella tendon)
• No soft tissue swelling
• No tibial fracture
• Normal alignment of Femur, Tibia and Fibula
17.
PLAN FOR MANAGEMENT
•Admit
• Regular diet
• Record v/s
• CBC, BUN, Cr, Electrolyte
• Tramol 50mg v q6hr
• Plasil 10mg v q6hr
• Paracetamol(500) 1 tab PO prn for pain q 4hr
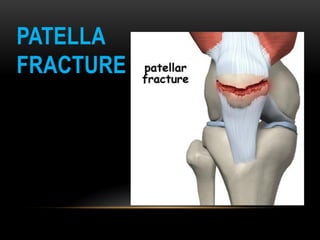
PATELLA FRACTURE
• Patellafractures account for 1% of all skeletal injuries
• male to female 2:1
• most fractures occur in 20-50 year olds
23.
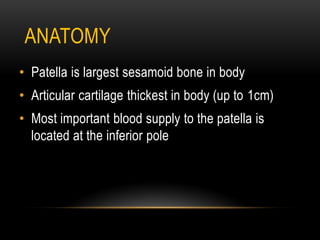
ANATOMY
• Patella islargest sesamoid bone in body
• Articular cartilage thickest in body (up to 1cm)
• Most important blood supply to the patella is
located at the inferior pole
24.
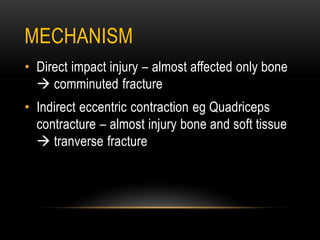
MECHANISM
• Direct impactinjury – almost affected only bone
comminuted fracture
• Indirect eccentric contraction eg Quadriceps
contracture – almost injury bone and soft tissue
tranverse fracture
PRESENTATION
• Anterior kneepain and swelling
• Non weight bearing
• palpable patellar defect
• significant hemarthrosis
• unable to perform straight leg raise indicates failure of
extensor mechanism (ไม่สามารถเหยียดหัวเข่า maintain ได้)
• retinaculum disrupted
27.
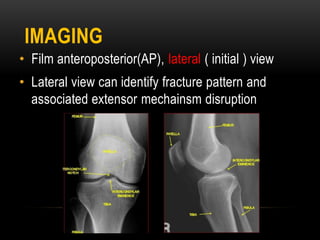
IMAGING
• Film anteroposterior(AP),lateral ( initial ) view
• Lateral view can identify fracture pattern and
associated extensor mechainsm disruption
28.
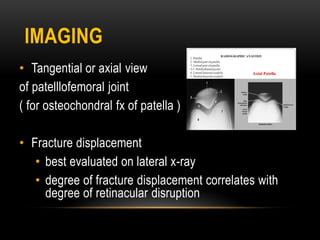
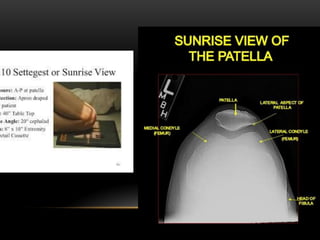
IMAGING
• Tangential oraxial view
of patelllofemoral joint
( for osteochondral fx of patella )
• Fracture displacement
• best evaluated on lateral x-ray
• degree of fracture displacement correlates with
degree of retinacular disruption
NON-OPERATIVE TREATMENT
knee immobilizedin extension (brace or cylinder cast)
and partial weight bearing in 6-8 weeks
indications
• intact extensor mechanism (patient able to perform
straight leg raise)
• nondisplaced or minimally displaced fractures
• vertical fracture patterns
--Follow up in 3 weeks: x-ray knee to check displaced--
--Rehabilitation program ROM after off cast 3-4 weeks--
33.
early active ROMwith hinged knee brace
• early WBAT in full extension
• progress in flexion
• after 2-3 weeks
NON-OPERATIVE TREATMENT
34.
OPERATIVE TREATMENT
ORIF withtension band construct
indications
• extensor mechanism failure (unable to perform
straight leg raise)
• fracture articular displacement >2mm
• displaced patella fracture >3mm
• open fractures
• preserve patella whenever possible
• patella sleeve fractures in children
35.
partial patellectomy
indications
• comminutedsuperior or inferior pole fracture
measuring <50% patellar height ONLY if ORIF is not
possible
techniques
• quadricep or patellar tendon re-attachment
• reattachment close to articular surface prevents
patellar tilt
• medial and lateral retinacular repair essential
36.
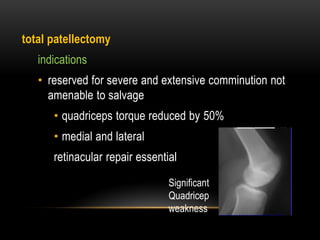
total patellectomy
indications
• reservedfor severe and extensive comminution not
amenable to salvage
• quadriceps torque reduced by 50%
• medial and lateral
retinacular repair essential
Significant
Quadricep
weakness
FOR THIS PATIENT
•ผู้ป่วยรายนี้ เมื่อดูจากอาการ ตรวจร่างกาย ทาให้ทราบได้ว่า ผู้ป่วย
มีอาการที่เข้าได้กับ fracture patella เพราะมีเข่าบวมแดง และ
เจ็บบริเวณด้านหน้าเข่า รูปทรงของ patella เปลี่ยนแปลง คลาได้
stepping และยังไม่สามารถยกขาขึ้นลอยค้างจากเตียงได้ (loss
of extensor mechanisim) ซึ่งบ่งบอก ว่าน่าจะมีการขาดของ
retinacular sleeve ด้วย
• จากแผ่นฟิล์ม X-ray left knee AP and lateral view : พบ มี
patella fracture แบบ transverse and joint stepping
39.
• วางแผนการรักษา จาเป็นต้องผ่าตัดแบบORIF with
tension band construct เนื่องจาก
-ผู้ป่วยมี ปัญหา loss of extensor mechanism
(unable to perform straight leg raise)
-ฟิล์มเจอ patella displaced มากกว่า 3 มม.
-patella bone เป็น sesamoid bone ที่ลอยอยู่ใน
intraarticular ทาให้การเชื่อมของกระดูกเป็นไปได้ไม่ดีนัก
-ผู้ป่ วยรายนี้ ฟิ ล์มเจอ joint stepping