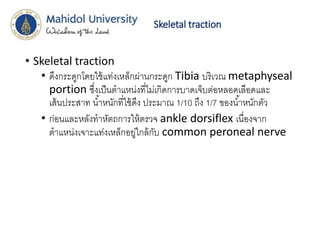
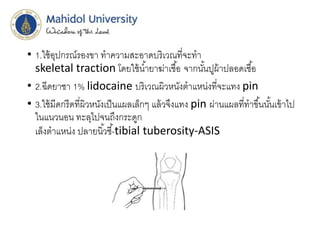
Primary survey
• A: can speak, can flex neck, not tender
along C-spine
• B : trachea in midline,equal chest movement,equal
and normal breath sound both lungs,CCT –ve
• C :BP 129/89 PR 90 /min , no external bleeding
• D : E4V5M6 pupil 3 mm RTLBE
6.
Primary survey
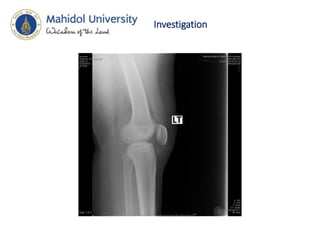
• E: swelling with tenderness and deformity of
Lt thigh,limit ROM of Lt hip due to pain,
multiple abrasion wounds size 3 cm and swelling of
Lt knee, ballotment –ve,not tender,DPA 2+,PTA2+,
can dorsiflexion and plantar flexion,normal pinprick
sensation
9.
Secondary survey
• A: no drug/food allergy
• M : no current medication
• P : no Hx. of surgery, no U/D
• L : last meal 15.00 น.
• E : 3 ชม. ก่อนมารพ. ขณะขี่รถจักรยานยนต์ ถูกรถยนต์ขับเบียด
ทาให้รถจักรยานยนต์ล้ม มีอาการปวดต้นขาซ้ายเป็นขึ้นมาทันที ขยับไม่ได้
ต้นขาซ้ายผิดรูป ไม่มีบาดแผลเลือดไหล สวมหมวกกันน็อค ไม่สลบ
จาเหตุการณ์ได้ ไม่มีอ่อนแรง ไม่มีอาการชา ญาตินาส่งรพ.
10.
Physical examination
• Head
Goodconsciousness , no wound
• Maxillofacial :
No wound
No facial deformity
• Cervical spine and Neck
C-Spine –can flex neck, not tender along
c-spine
Neck –No stridor , No hematoma
11.
Physical examination
• Chest
Tracheain midline,equal and normal breath
sound both lungs , CCT –negative , no wound,
no subcutaneous emphysema, RR 18/min
• Abdomen
soft , not tender
• Perineum
No wound , no ecchymosis,PCT - negative
• Neurologic
E4V5M6 , pupil 3 mm RTLBE
Motor gr. V all extremities except Lt lower
extremities can’t evaluate due to pain
12.
• Extremities :
swellingwith tenderness and deformity of
Lt thigh,limit ROM of Lt hip due to pain,
multiple abrasion wounds size 3 cm and swelling of
Lt knee, ballotment –ve,not tender,DPA 2+,PTA2+,
can dorsiflexion and plantar flexion,normal pinprick
sensation
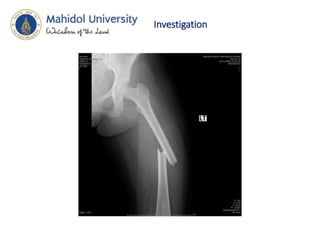
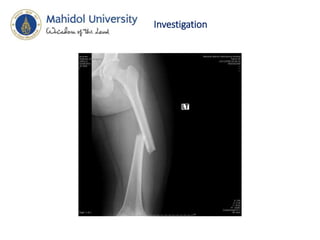
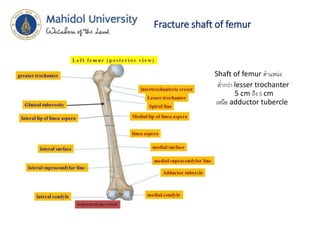
Fracture shaft offemur
• Shaft of femur ตาแหน่ง
• ต่ากว่า lesser trochanter
5 cm ถึง 5 cm
เหนือ adductor tubercle
20.
Fracture shaft offemur
• Mechanism
• traumatic
• high-energy
• most common in younger population
• often a result of high-speed motor vehicle accidents
• low-energy
• more common in elderly
• often a result of a fall from standing
• gunshot
21.
Fracture shaft offemur
• Associated conditions
• ipsilateral femoral neck fracture
• 2-6% incidence
• often basicervical, vertical, and nondisplaced
• bilateral femur fractures
• significant risk of pulmonary complications
• increased rate of mortality as compared to unilateral fractures
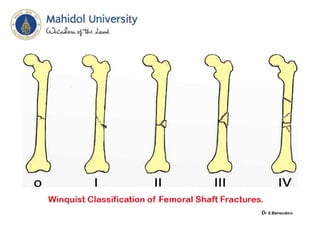
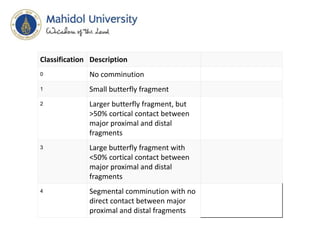
Classification Description
0 Nocomminution
1 Small butterfly fragment
2 Larger butterfly fragment, but
>50% cortical contact between
major proximal and distal
fragments
3 Large butterfly fragment with
<50% cortical contact between
major proximal and distal
fragments
4 Segmental comminution with no
direct contact between major
proximal and distal fragments