Primary survey
• A: able to talk , not tender at posterior c spine , full ROM
of neck
• B : equal breath sound both lung , CCT negative
• C : V/S BP 143/85 mmHg PR 77 bpm , no active external
wound bleeding
• D : E4V5M6 pupil 3 mm RTLBE
• E : no external wound , no open fracture , Lt wrist
deformity limit ROM due to pain
6.
Secondary survey
• A: no food or drug allergy
• M : no current medication
• P : no underlying disease
• L : last meal 13.00 pm
• E : 3 hr ก่อนมารพ ขณะผู้ป่วยเล่นฟุตบอล ตาแน่งผู้รักษาประตู ได้เอามือปัดลูกฟุตบอล
หลังจากนั้น ข้อมือข้างซ้ายผิดรูป ปวดข้อมือทันที ข้อมือบวม ไม่ชา ขยับนิ้วได้ ไม่มีแผลเปิด
7.
Physical examination
• Generalappearance : A middle aged Thai man, good
consciousness, well co-operative
• V/S : BP 143/85 mmHg, PR 77 bp, BT 36.5, RR 18 /min
• HEENT : no ple conjunctivae, anicteric sclerae
• Heart : normal S1 S2 no murmur
• Lung : normal breath sound equal both lung
8.
Physical examination
• Extremities: Lt wrist
• no external wound
• mild swelling with deformity
• marked tender at radial side
• limit ROM due to pain
• cap refill < 2 sec, radial pulse 2+
• good pinprick sensation
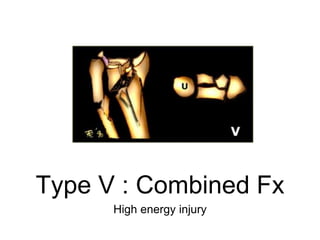
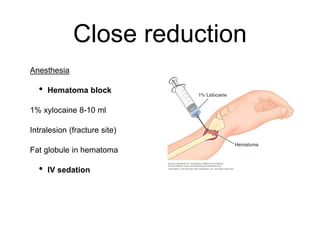
Treatment
• Goal
• Preservehand and wrist function
• Realign normal osseous anatomy (articular surface)
• Promote bony healing
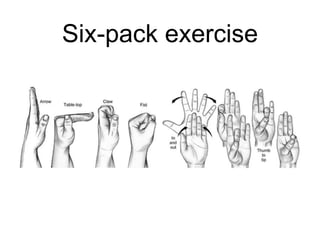
• Allow early finger and elbow ROM
35.
Treatment
• Non operative
•Close reduction and cast immobilization
• Indication
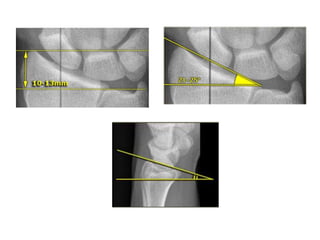
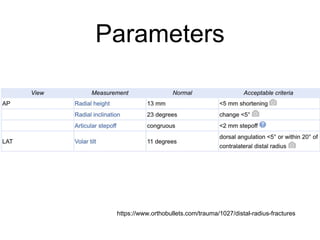
1. Extra articular
2. Radial shortening < 5 mm
3. Dorsal angulation < 5 or within 20 of
contralateral distal radius
After reduction
• Immobilizedby slab (short arm /long arm) with wrist in
neutral position
• Check X ray confirm to acceptable reduction
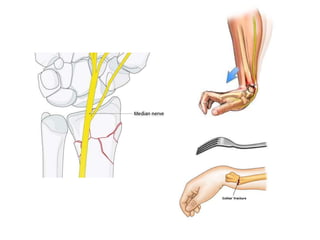
• Watch median nerve symptoms
• Follow up x ray needed in 1-2 wk to evaluated reduction
• Change to short arm cast after 2-3 wk ,continue until
fracture healing
40.
After reduction
• Outcome
•Repeat closed reductions have 50% less than
satisfactory results
• Complication
• Acute carpal tunnel syndrome
• EPL rupture
41.
Treatment
• Operative
• Indication
•(Unstable)
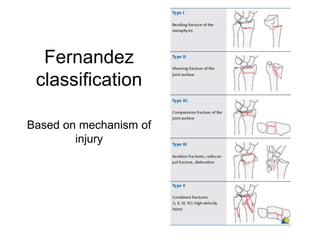
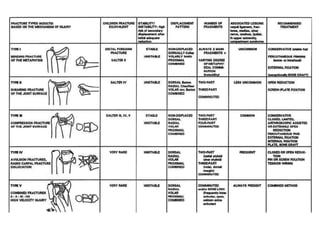
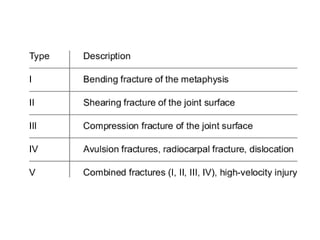
1. Fernandez type II,IV,V and some in I,III
2. Lafontaine criteria 3 of 5 instability parameters
3. Secondary displacement after casting
• Unacceptable alignment(after reduction)
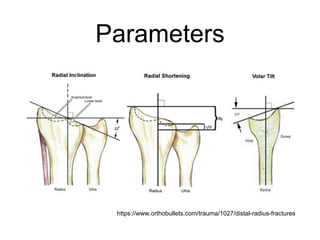
• Radial inclination < 15
• Shortening > 5 mm
• Dorsal tilt > 10
• Volar tilt > 20
• Articular step off or gap > 2 mm
Indication for surgery
44.
Indication for surgery
•Open fracture
• Irreducible fracture
• Double die punch
• Displaced comminuted PM fragment
• Articular step off > 2 mm
• Severe comminution
• Shortening > 5 mm