Downloaded 1,103 times

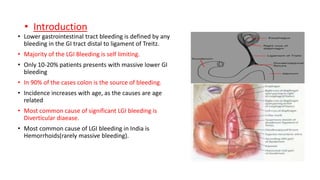






















Lower gastrointestinal tract bleeding can be caused by various conditions affecting the colon and small intestine. The most common cause is diverticular disease, followed by hemorrhoids. Bleeding may present as hematochezia, melena, or occult bleeding resulting in anemia. Colonoscopy is the primary diagnostic tool for evaluating the source and managing bleeding, while other modalities like capsule endoscopy and angiography can also be used. Treatment depends on the underlying cause and may involve endoscopic therapies, medications, or surgery.











































































































