LEARNING OBJECTIVES
• Definelower GI bleeding.
• Understand the various presentations of lower GI bleeding
• Consider the various classifications of lower GI bleeding
• The causes of lower GI bleeding
• Investigations for lower GI bleeding
• Treatment of lower GI bleeding
• Briefly consider the common causes of lower GI bleeding
3.
INTRODUCTION
• Lower gastrointestinaltract bleeding is defined as any bleeding in the Gl tract distal to
ligament of Treitz.
• Majority of the LGI Bleeding is self limiting.
• Only 10-20% patients presents with massive lower GI bleeding
• In 90% of the cases colon is the source of bleeding.
4.
INTRODUCTION
• LGIB:
• Incidenceincreases with age, as the causes are age related
• Most common causes of significant LGI bleeding are Haemorrhoids and
Diverticular disease.
• Most common cause of LGI bleeding in general is Haemorrhoids(rarely massive
bleeding).
5.
DEFINITION
• Lower GI- bleeding is defined as abnormal haemorrhage into the lumen of the bowel from
a source distal to the ligament of Treitz.
• Normal faecal blood loss - 1.2 ml / day
• Significant - > 10 ml / day
6.
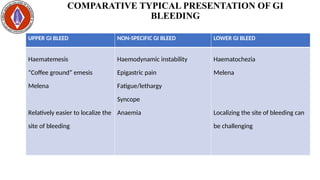
COMPARATIVE TYPICAL PRESENTATIONOF GI
BLEEDING
UPPER GI BLEED NON-SPECIFIC GI BLEED LOWER GI BLEED
Haematemesis
“Coffee ground” emesis
Melena
Relatively easier to localize the
site of bleeding
Haemodynamic instability
Epigastric pain
Fatigue/lethargy
Syncope
Anaemia
Haematochezia
Melena
Localizing the site of bleeding can
be challenging
7.
PRESENTATION
• Lower Glbleeding typically presents with:
• Haematochezia (which can range from bright-red blood to old clots)
• Melena (If the bleeding is slower or from a more proximal source)
• Abdominal/Anal pain
• Features of anaemia
• Features of shock (In massive haemorrhage)
8.
INCIDENCE
• LGIB constituteabout 20-33% of episodes of gastrointestinal (GI)
haemorrhage.
• The incidence rises steeply with advancing age.
• 80% may resolve spontaneously.
• 25% may re-bleed.
9.
PRINCIPLES IN THEMANAGEMENT OF
LGIB
• Assess and classify the amount of blood loss
• Replace the blood loss volume for volume(Resuscitation)
• Diagnose the cause through investigations
• Treat the cause(s) adequately
10.
CATEGORIZATION OF (LGI)BLEEDING BY INTENSITY
• Massive bleeding
• Moderate bleeding
• Occult bleeding
11.
MASSIVE BLEEDING
• Patientpresents with passage of large volume of bright red blood PR
• Bleeding > 1.5 l/ day
• Hemodynamic instability & shock
• Shock Index (SI) of 1 and above signifies severe haemorrhage.(SI = HR/SBP)
• Normal SI ranges between 0.5 to 0.7
• Decrease in haematocrit level of 6 g / dL
• Transfusion of at least 2 units of packed red blood cells
• Bleeding that continues for 3 days
• Common causes
• Diverticulosis / Angiodysplasia/Haemorrhoids (Occasionally)
12.
MODERATE BLEEDING
• Presentsas haematochezia or Malena*
• Hemodynamically stable
• Shock index is near normal
• Initial decrease in haematocrit level of 8 g / dL or less
• Causes
• Ano-rectal / Congenital / Inflammation & Neoplastic diseases
13.
OCCULT BLOOD
• Occursin the setting of a positive FOBT and/or iron deficiency anaemia.
• Iron deficiency anaemia has traditionally been attributed to chronic occult GI
bleeding
• Detected by routine chemical tests of the stool, with or without systemic
evidence of chronic blood loss.(Tiredness, Weakness, Shortness of
breath, Dizziness or light-headedness).
• 10 ml. of blood loss / day is necessary to have stool occult blood positive.
WITH PAIN
• Fissure-in-Ano
•Fistula-in-Ano
• Ca. Anal Canal
• Rup. perianal haematoma
• Rup. Ano Rectal abscess
• Endometriosis
• Injury
18.
WITHOUT PAIN
• BloodAlone
• Polyp
• Villous Adenoma
• Diverticular diseases
• Blood After Defecation
• Haemorrhoids
• Blood with mucus
• Ulcerative colitis
• Intussusception
• Ischaemic Colitis
• Blood Streaked on stool
• Ca. Rectum
19.
MNEMONIC TO REMEMBERTHE MAJOR
CAUSES OF LGIB
• NADIR
• N – Neoplasms (Benign or Malignant)
• A – Angiodysplasias/arteriovenous malformations
• D – Diverticulosis, Dyscraysias, Drugs (NSAID/Anticoagulant)
• I – Inflammatory bowel diseases (Crohn’s, Ulcerative colitis), infections
• R – Rhoids Haemorrhoids and/or fissure-in-Ano
20.
CLINICAL PRESENTATIONS
Bleeding Perrectum:
Bright red blood Haemorrhoids (Piles) / Polyps / Fissure
Altered blood Ca / Ulcer / IBD / Dysentery
Maroon colour Meckel's diverticulum
Streaks of blood Anal fissure
Splash in pan Haemorrhoids (Piles)
Red currant jelly Intussusception
Blood with mucus Colitis / Ca / Dysentery
Note: Ask & Look for bleeding tendency.
21.
RELATION TO DEFECATION
•Streak of fresh blood – Fissure-In-Ano
• When passing stool - Bright red & Splashes over the pan
- Haemorrhoids (Piles)
• Other than during defecation - Polyps / PP / RP / Ca / UC
• Bleeding per anum in child - Polyp
22.
OTHERS SYMPTOMS ANDSIGNS
• Pain
• Altered bowel habits
• Anaemia / Malnutrition / Loss of Weight I Loss of Appetite
• Mass palpable PA - Rt /Lt
• Per-rectal exam - Very important
23.
LOCALIZATION OF THEBLEEDING SITE
• Is a major challenge in the management of LGIB
• In about 10% of patients presenting with lower
gastrointestinal bleeding (LGIB), the source of bleeding is
from the upper gastrointestinal (GI) tract.
24.
LOCALIZATION OF THEBLEEDING SITE
• Some patients with LGIB should have a nasogastric (NG) tube placed:
• if the aspirate or lavage does not show any blood or coffee ground material, upper GI
tract is unlikely.
• In case of high suspicion, obtain an esophagogastroduodenoscopy (OGD)
evaluation
• Complete lower GI evaluation investigations should the be carried out to
locate the site of bleeding
25.
INVESTIGATIONS
• Aims at:
•Confirming that there is GI bleeding
• Locate the site of the bleeding
• Arrive at a definitive cause/diagnosis
• May also serve as both investigation and treatment.
COLONOSCOPY
• Diagnostic usesare
• Visualization of the lesion
• Biopsy of the lesion
• Therapeutic uses are
• Electro-cauterization of bleeding points
• Polypectomy
INVESTIGATIONS - CONTD
•Abdominal USS – Tumour/Tumour Metastasis
• Mesenteric Angiography
• In this procedure bleeding rate of 0.5-1ml/ min can be detected.
• Selective angiography is done by catheterising the arteries
selectively under fluoroscopic guidance.
• Therapeutic application can be achieved by embolization of the
culprit vessel
• Angiodysplasia / Tumours/ Vasculitis – Can be diagnosed
34.
RADIONUCLEOTIDE SCANNING (Tc-99MLABELLED RBC
SCINTIGRAPHY)
• A sample of patient's blood is taken and then the RBC of the sample is
labelled with Tc-99m.
• Next the sample of blood is injected into the patient and serial scintigraphy
scan are taken in fixed intervals.
• It only has diagnostic purpose. But the advantage is that it can detect very
small amount of bleeding(0.05-0.1 ml/min)
CAPSULE ENDOSCOPY
• Noninvasive procedure
• Done in stable patients
• Duration is 8h/50000 images
• Only diagnostic value
• The imaging cannot be controlled from outside, thus pathological site may be
missed
38.
RESUSCITATION AND INITIALASSESSMENT
• Initial evaluation and hemodynamic resuscitation:
• Obtain a focused history, physical examination, and laboratory studies at the time of
patient presentation (to determine severity, potential causes and site),
• while concurrently performing hemodynamic resuscitation.
• In the presence of haematochezia and hemodynamic instability, where an upper
gastrointestinal bleeding (UGIB) site is suspected:
• Perform an upper endoscopy or
• Use nasogastric aspirate/lavage to help role out/determine a potential upper GI source.
39.
RESUSCITATION AND INITIALASSESSMENT
• Perform risk assessment and stratification.
• Administer intravenous (IV) fluid resuscitation in patients with
hemodynamic instability and/or suspicion of active bleeding.
• Transfuse packed red blood cells (PRBCs) to maintain the
haemoglobin level above 7 g/dL.
40.
INITIAL RESUSCITATION -ACTION
• Establish large-bore IV access and administer normal saline.
• Routine laboratory studies (e.g., complete blood cell (CBC) count, electrolyte,
and coagulation studies),
• Blood should be typed and cross-matched.
• The patient's blood loss and hemodynamic status should be ascertained, and in
cases of severe bleeding,
• The patient may require invasive hemodynamic monitoring (CVP, PCWP) to direct
therapy.
41.
INITIAL RESUSCITATION
• Patientsin shock should receive fluid volume replacement without delay.
• Colloid or crystalloid solutions may be used to achieve volume restoration
before administering blood products.
• PRBC transfusions should maintain the haemoglobin level above 7 g/dL,
with a threshold of 9 g/dL in those with massive bleeding or
• Significant comorbid conditions, or
• If there may be a delay in more definitive treatment
42.
TRANSFER TO INTENSIVECARE UNIT
• Patients who may require admission to the intensive care unit and early
involvement of both a gastroenterologist and a surgeon include the following:
• Patients in shock
• Patients with continuous active bleeding
• Patients at high risk, such as patients with
• Serious comorbidities,
• Those needing multiple blood transfusions, or
• Those with an acute abdomen
43.
TREATMENT
• Identified Causeis treated, but sometimes no definite cause/location of bleeding can be
identified.
• Treatment can be either endoscopic or open (Laparotomy)
• Proper exploration - lengthy midline incision – essential if the bleeding site is not certain
• Polyps: Endoscopic polypectomy
• Mesenteric ischemia: Massive resection - small bowel
• Colonic carcinoma: Surgical resection as appropriate to the location of the tumour.
44.
TREATMENT
• Sigmoid diverticula:
•Sigmoid colectomy/Total colectomy may be carried depending on the extend of the disease.
• Angiodysplasia:
• Endoscopic fulguration / Therapeutic embolization / Hemicolectomy
• Ulcerative colitis:
• Drugs {Mesacol (Mesalazine)} enema / Total proctocolectomy and anastomosis
• Haemorrhoids (Piles):
• Appropriate haemorrhoidectomy procedure
45.
BRIEF DISCUSSION OFFEW OF THE CAUSES OF
LGIB
• Anorectal dieases: Haemorrhoids
• Diverticular disease
• Colitis
• Angiodysplasia
46.
ANORECTAL DISEASES
• Haemorrhoid:-
•These are cushions of submucosal tissue containing venules, arterioles, smooth muscle fibre
& elastic connective tissues
• 3 anal cushions are found in 3,7&11 o'clock position in anal canal.
• Caused by increased intra abdominal pressure i.e.
• Obesity
• Constipation
• Pregnancy
• Straining to pass urine
47.
ANORECTAL DISEASES
• Internalhaemorrhoids - located proximal to dentate line
• Usually painless, thus banding, ligation can be done.
• External haemorrhoids - located distal to dentate line
• These are painful, usually self limited.
• Classification of internal haemorrhoids and treatment
48.
ANORECTAL DISEASES
• Sclerotherapyis done by 5% phenol in almond or arachis oil
• Operative haemorrhoidectomy are done by:
• Milligan-Morgan's open haemorrhoidectomy,
• Ferguson closed haemorrhoidectomy,
• Whitfield submucosal haemorrhoidectomy,
• Long's stapler method.
49.
DIVERTICULAR DISEASE OFLGI TRACT
• Next most common cause of significant LGI bleeding after haemorrhoid.
• Incidence increases with age
• Prevalent in western countries and developing countries where the dietary fibres in the
food is less in amount.
• Less dietary fibre causes increased duration of transit time followed by increased
intraluminal pressure.
• This results in diverticulum (pulsion type)
50.
DIVERTICULAR DISEASE OFLGI TRACT
• Caused by mucosal outpouching at the site of entrance of vessel i.e.
Appendices epiploicae of the colon.
• Present on the anti mesenteric border of LGI tract
• Bleeding occurs in 3-15% of patient with diverticulosis
• More than 75% of bleeding stops spontaneously with 10% rebleeds in 1year
and 50% in 10 years.
DIVERTICULAR DISEASE OFLGI TRACT
• Diverticulitis - is infected diverticula due to impaction of faecal material
at neck and result into perforation/intraperitoneal
abscess/peritonitis/LGI bleeding/ fistula.
• Best method of diagnosis-Full length colonoscopy/Ba enema
• Indication of surgery in Diverticulitis are
• No improvement in medical therapy
• At least 2 documented attacks of diverticulitis
• Complicated diverticulitis
• Recurrent or persistent haemorrhage.
53.
DIVERTICULAR DISEASE OFLGI TRACT
• Therapeutic use of colonoscopy is done to control bleeding by
• Epinephrine injection
• Electrocautery
• Endoscopic clips.
• If haemorrhage recurs then colonic resection is indicated.
Surgical Specimen
of Diverticulosis
Barium Enema
showing Diverticuli
54.
COLITIS
• An inflammatoryreaction in the colon, often auto-immune or infectious.
• Most common types
• Ulcerative colitis
• A chronic, inflammatory bowel disease that causes inflammation in
the digestive tract
• Crohn's disease
• A chronic inflammatory bowel disease that affects the lining of the
digestive tract.
• C. Diff. Colitis
• Inflammation of the colon caused by the bacteria Clostridium
difficile.
55.
COLITIS
• Both infective/inflammatorycolitis present as LGI bleeding, mostly
haematochezia, pus may also be present.
• DIAGNOSIS
• The diagnosis of Ulcerative colitis and Crohn's disease is usually confirmed
by biopsies on colonoscopy.
• Although colonoscopy and sigmoidoscopy are still employed, now stool
testing for the presence of C. difficile toxins is frequently the first-line
diagnostic approach with history of prior antibiotic use or hospitalization.
56.
ANGIODYSPLASIA
• Angiodysplasia isa small vascular malformation of the gut.
• It is a common cause of otherwise unexplained gastrointestinal
bleeding and anaemia.
• Cases present with black, tarry stool (melena), the blood loss can be
subtle, with the anaemia symptoms predominating
57.
ANGIODYSPLASIA
• Diagnosis ofangiodysplasia is often accomplished with colonoscopy or
esophagogastroduodenoscopy (EGD).
• Treatment may be with:
• Colonoscopic interventions,
• Angiography and embolization,
• Medication, or
• Occasionally surgery.
CONCLUSION
• Lower gastrointestinalbleeding (LGIB)
• 10-20% may present with massive bleeding.
• In 90% of cases, the source of the bleeding is the colon.
• Incidence increases with age.
• Majority of the cases are self-limiting.
• Resuscitation is paramount in massive LGIB, before diagnosis and any
definitive treatment.
• Outcome of management will depend on the cause of the bleeding, but
generally, the outcome is good.