Downloaded 387 times


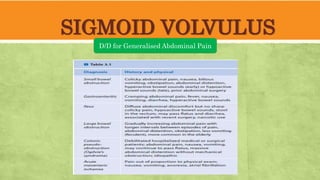
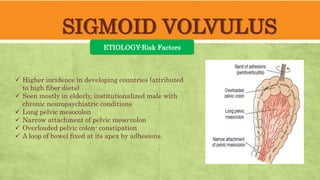


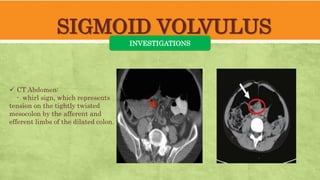
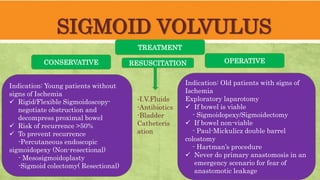
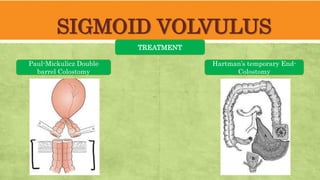
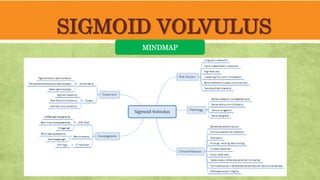
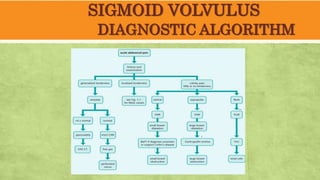
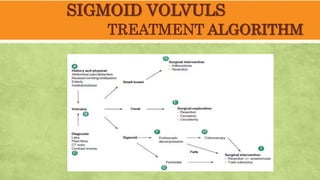


This document provides an overview of sigmoid volvulus, a condition characterized by twisting of a segment of the colon, leading to obstruction. It discusses its epidemiology, risk factors primarily affecting the elderly, clinical features, differential diagnosis, and investigative techniques. Treatment approaches vary based on patient age and ischemia signs, including endoscopic and surgical options, emphasizing the need for resuscitation and careful management to prevent complications.























































































