This document discusses lower gastrointestinal (GI) bleeding, including:
1. Definitions of lower GI bleeding and what constitutes significant bleeding. Lower GI bleeding originates in the small or large intestine.
2. Presentations of lower GI bleeding ranging from hematochezia to melena to occult bleeding. Massive bleeding presents as hemodynamic instability while moderate bleeding is stable.
3. Common causes of lower GI bleeding including diverticular disease, inflammatory bowel disease, angiodysplasia, and cancers. Local causes depend on specific sites within the intestines.
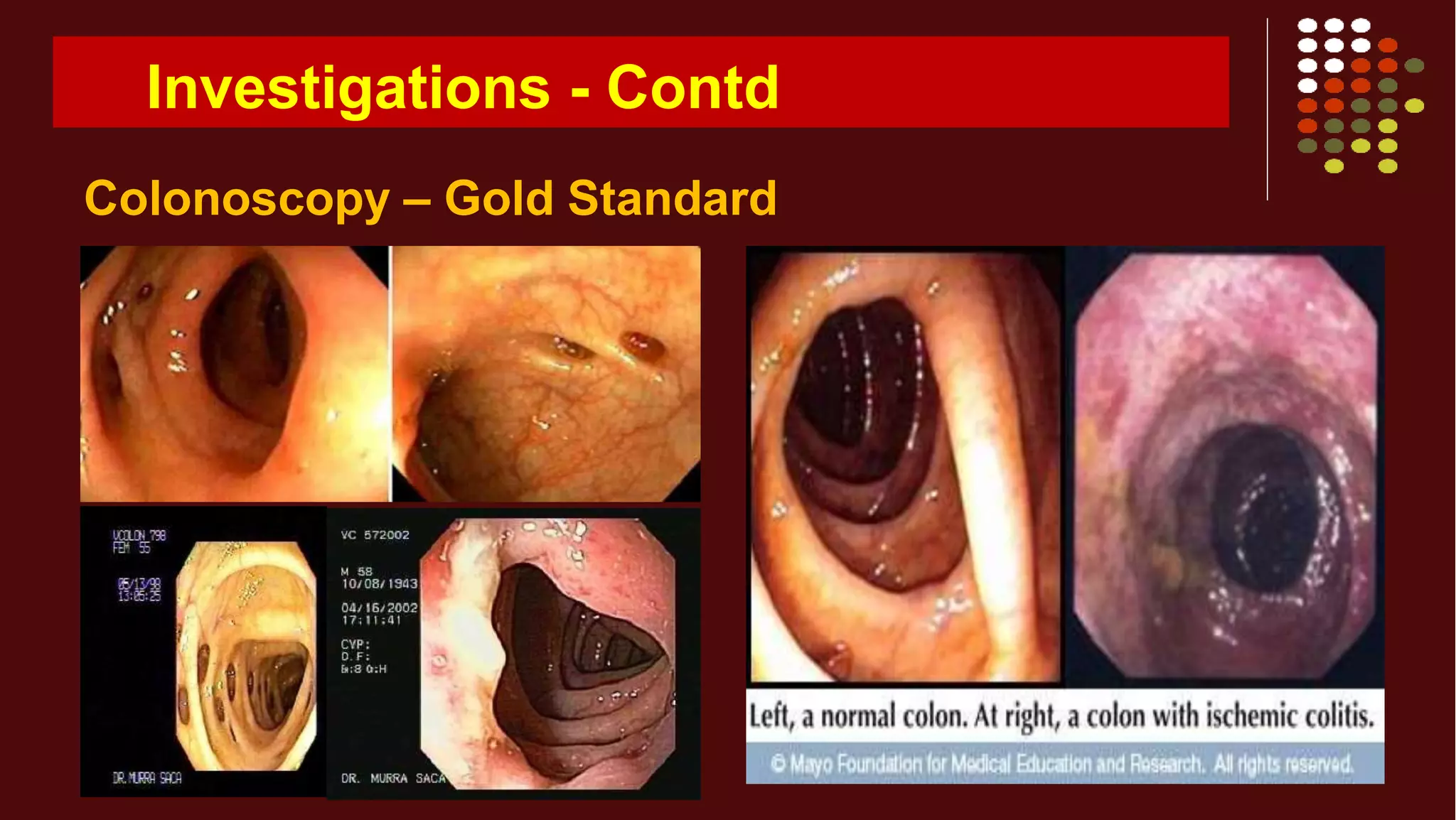
4. Evaluations include blood tests, stool tests, imaging like colonoscopy, and in some cases angiography to localize the source and