Downloaded 227 times
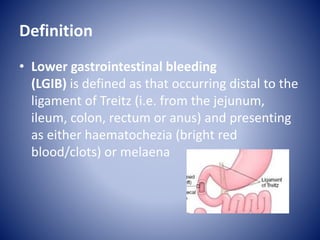



































This document discusses lower gastrointestinal bleeding (LGIB), which occurs in the small and large intestines, presenting as hematochezia or melaena. Common causes of LGIB include diverticular disease, inflammatory bowel diseases like Crohn's disease and ulcerative colitis, ischemic colitis, vascular malformations, polyps, tumors, and anal issues. LGIB is typically chronic and self-limiting, though some cases are acute and require blood transfusion. The diagnostic workup depends on the patient's age and symptoms, and may involve endoscopy, imaging, or angiography to identify the source of bleeding.






















































































