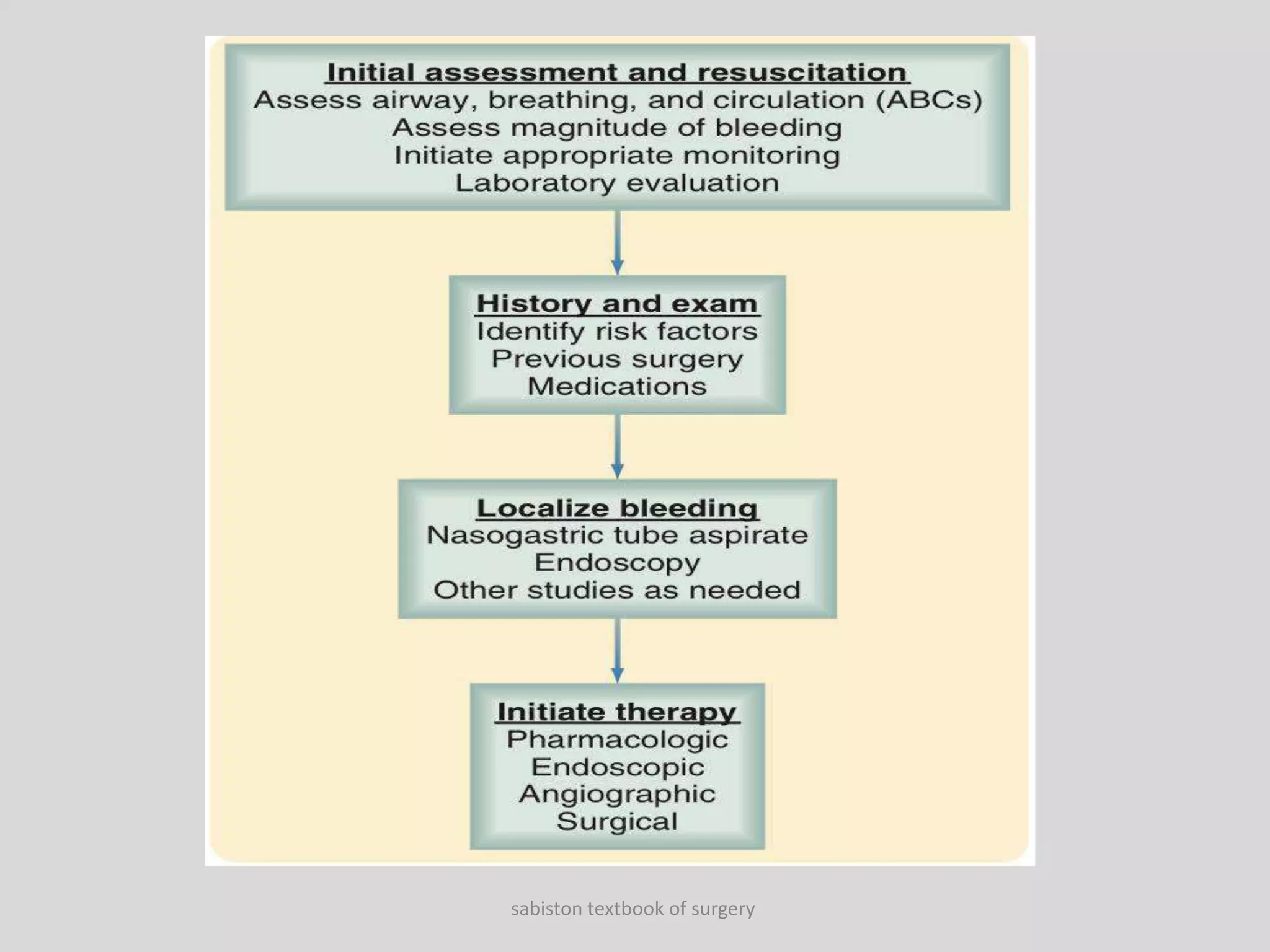
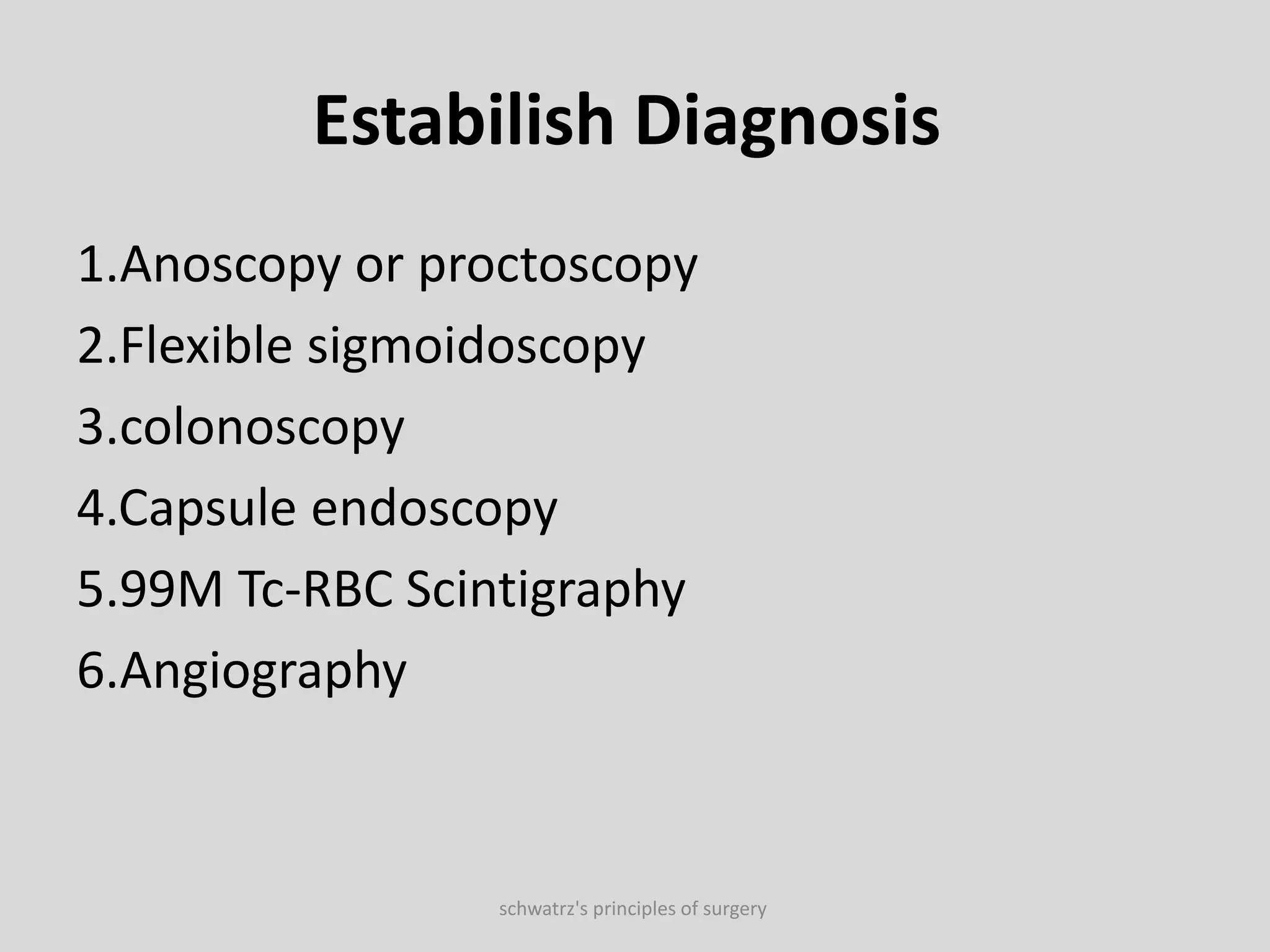
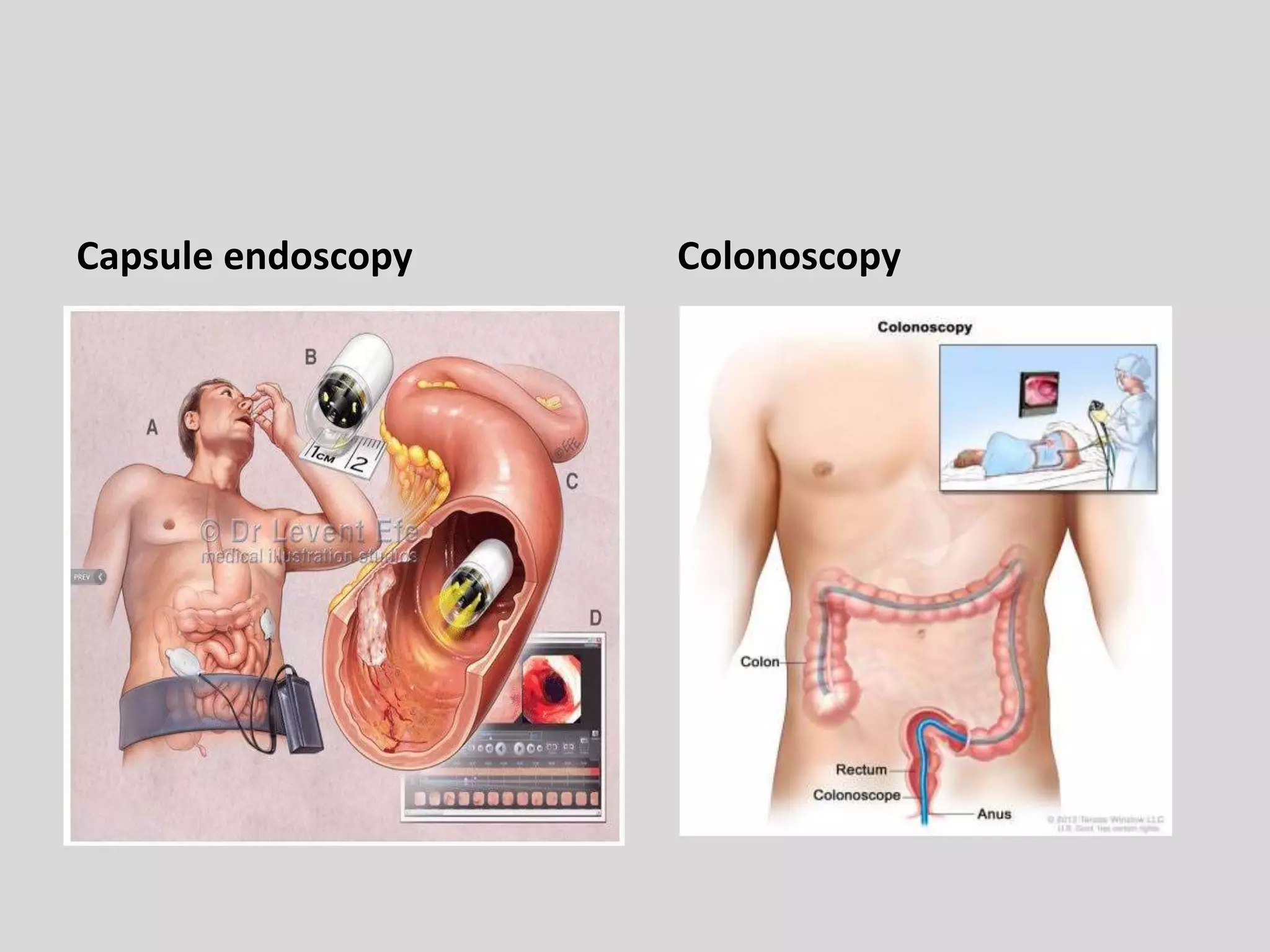
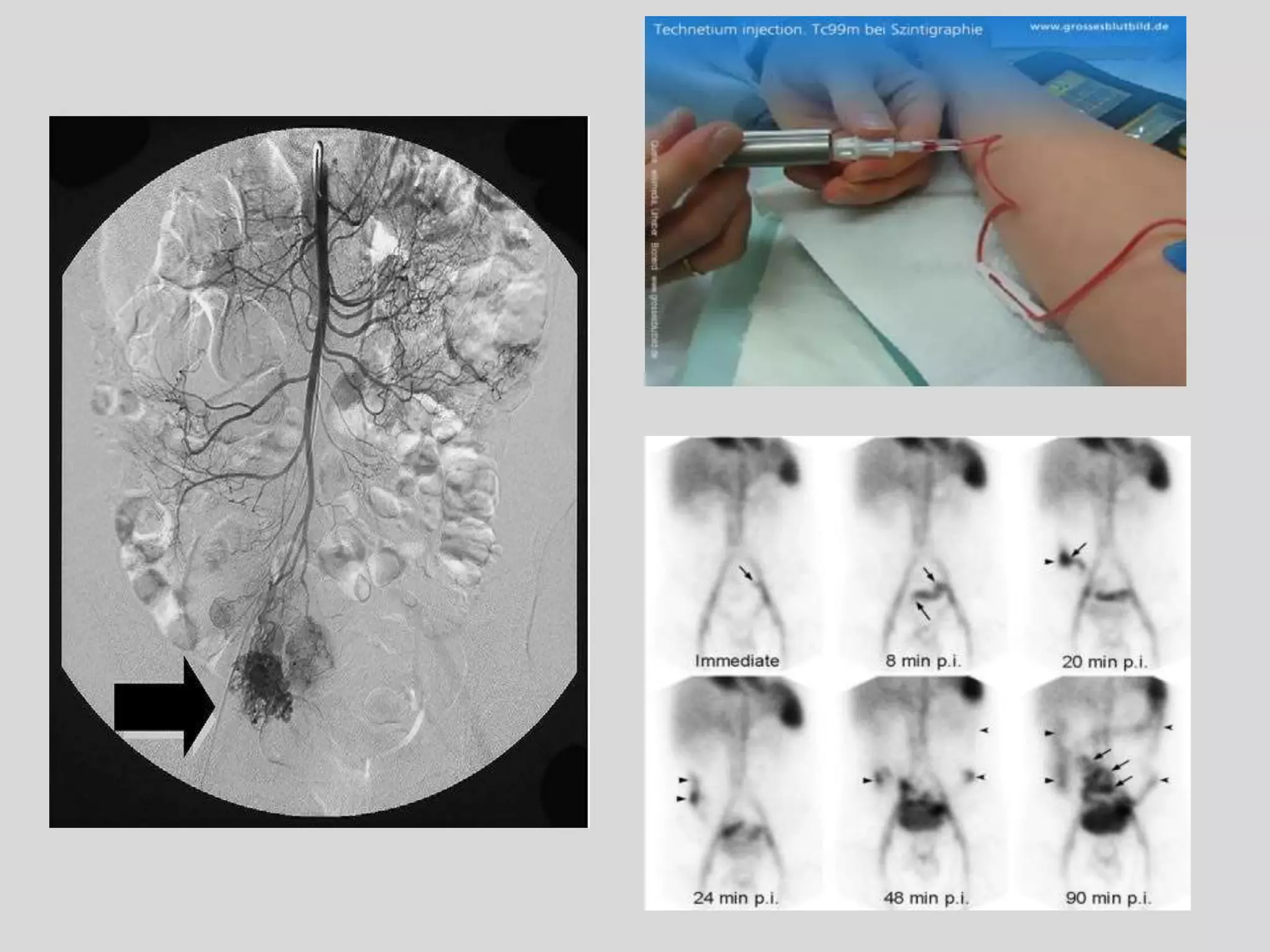
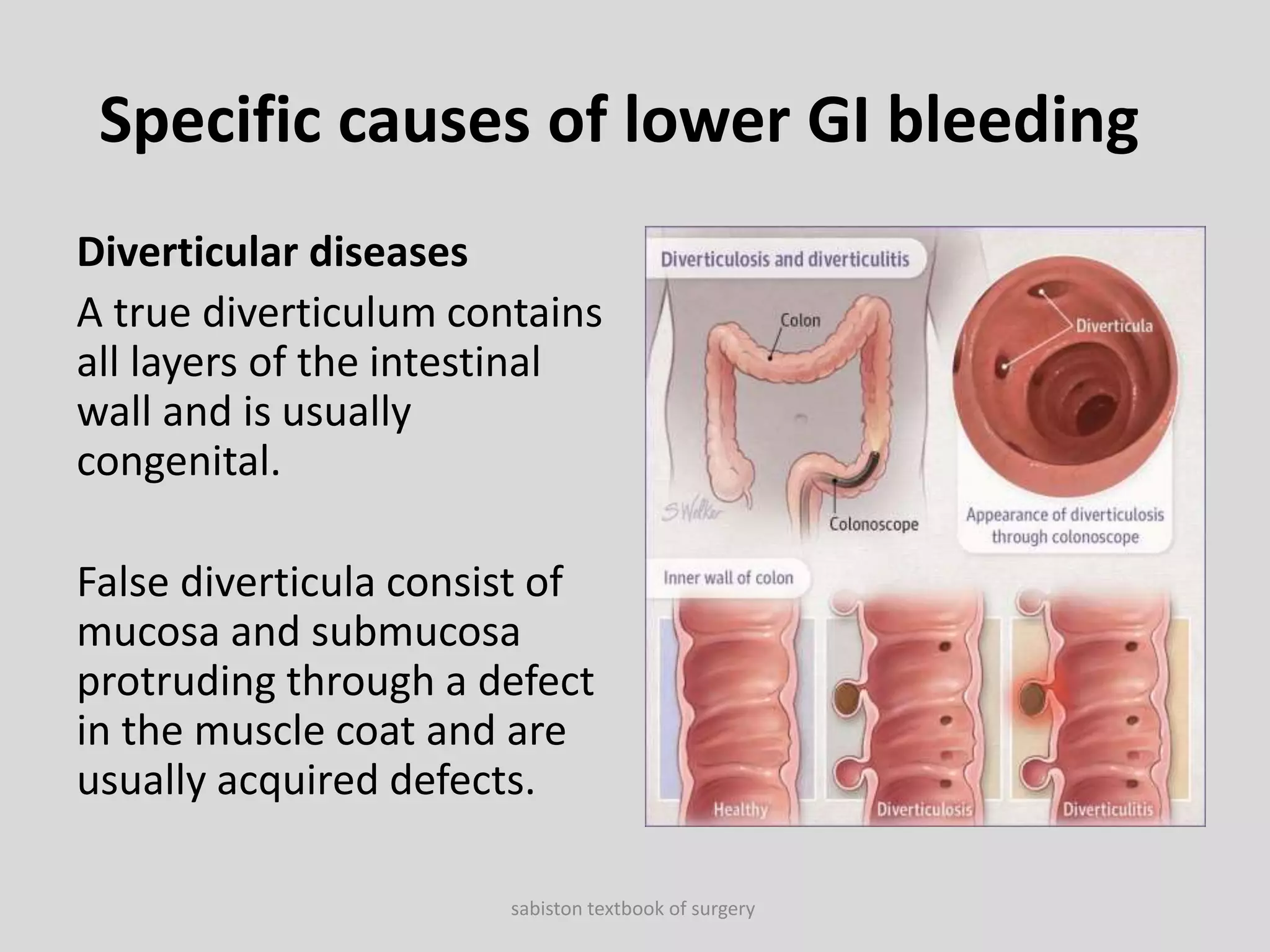
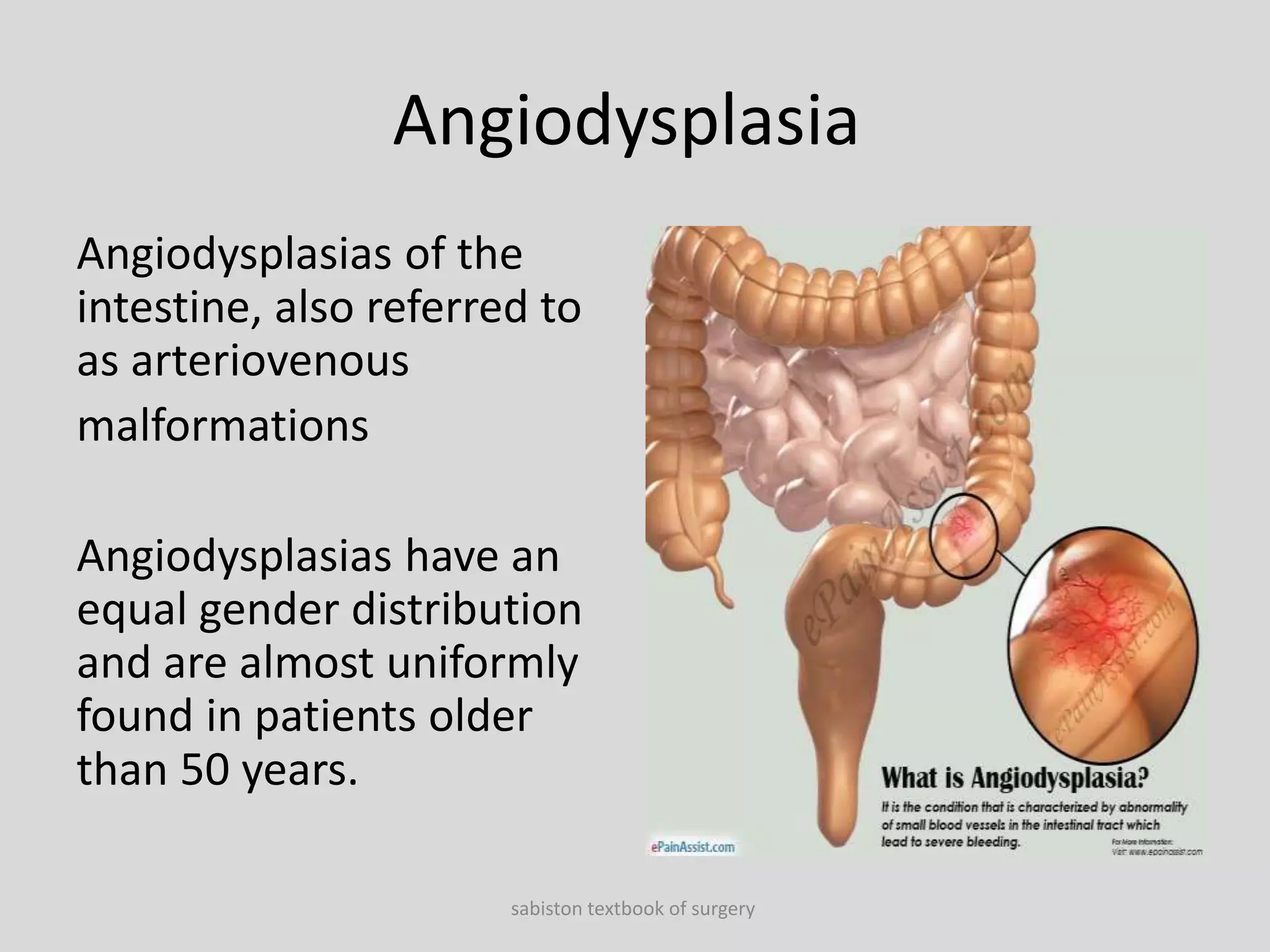
This document discusses lower gastrointestinal (GI) bleeding, which originates in the small or large intestine. Lower GI bleeding accounts for 20-33% of GI hemorrhages and can present with maroon or bright red stools depending on the bleeding source. Causes of lower GI bleeding include diverticular diseases, anorectal diseases like hemorrhoids and anal fissures, colorectal neoplasms, polyps, colitis, inflammatory bowel disease, and angiodysplasias. Management involves resuscitation, diagnostic tests to localize the bleeding source like endoscopy, and potentially surgery to control or resect the bleeding area.