Downloaded 349 times
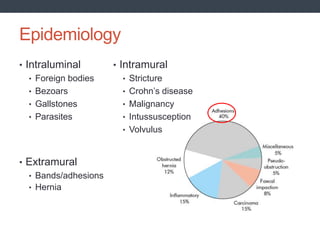
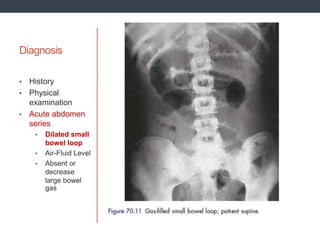
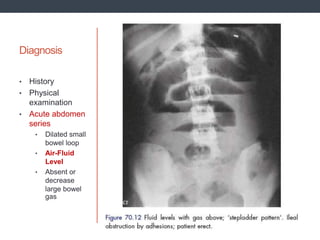
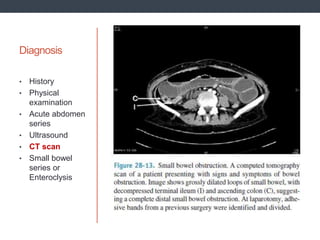
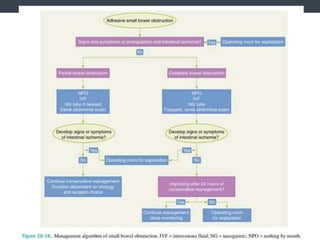

Small bowel obstruction can occur due to various intraluminal, extramural, or intramural causes that obstruct the lumen. The clinical manifestations include abdominal pain, vomiting, distension, and constipation. Diagnosis involves history, physical exam, abdominal x-rays showing dilated small bowel loops and air-fluid levels. Management depends on the severity and includes supportive care, surgery for complete or strangulated obstructions, or potentially conservative management for some inflammatory causes.























































































