Downloaded 641 times
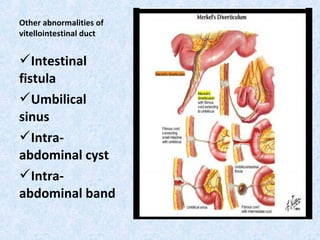
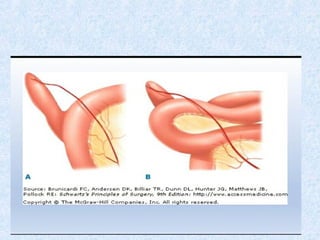
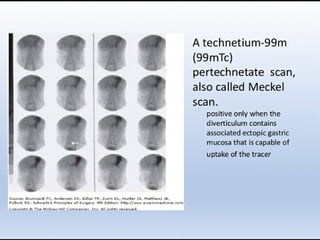


Meckel's diverticulum is the most common congenital abnormality of the gastrointestinal tract, occurring in approximately 2% of the population. It results from incomplete obliteration of the vitelline duct during fetal development. While most cases are asymptomatic, Meckel's diverticulum can cause complications like bleeding, diverticulitis, intestinal obstruction, and intussusception due to heterotopic gastric or pancreatic tissue. Diagnosis is often made through scans like a technetium-99m pertechnetate scan or CT scan. Treatment involves surgical resection of the diverticulum and adjacent bowel segment for symptomatic cases.























































































