Downloaded 652 times
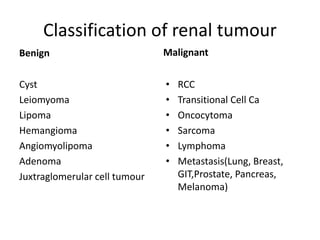

This document summarizes renal cell carcinoma (RCC), the most common type of kidney cancer. Key points include: - RCC originates in the renal cortex and arises mostly from the upper pole of the kidney. - Common subtypes include clear cell, papillary, and chromophobe carcinomas. - Risk factors include male sex, older age, smoking, obesity, and genetic conditions like von Hippel-Lindau syndrome. - Symptoms may include hematuria, flank pain, and palpable flank mass. Imaging like CT and MRI are used to diagnose and stage disease. - Treatment depends on stage but typically involves surgical removal (radical or partial nephrectomy











































































































