Download to read offline



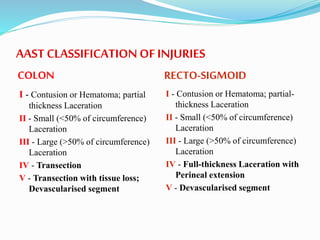
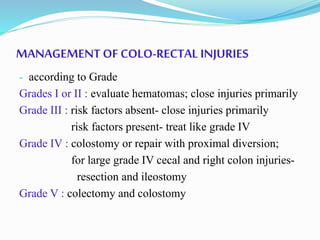


The document discusses colorectal trauma management with detailed case studies illustrating blunt abdominal injuries, their diagnosis, surgical interventions, and post-operative care. It highlights the low incidence of colorectal injuries in blunt trauma, classifies such injuries according to the AAST criteria, and outlines management strategies based on injury grades. Two specific cases demonstrate the intricacies of diagnosis and treatment, emphasizing the potential complexities of colorectal injuries in trauma patients.






















































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)
