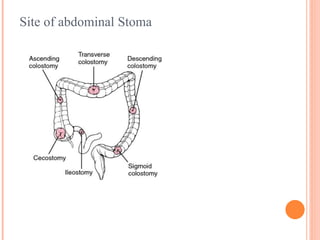
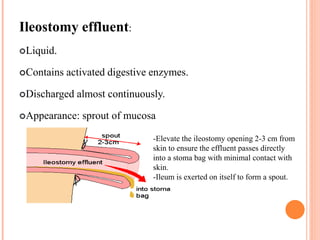
An intestinal stoma is an artificial opening in the abdominal wall that connects the intestinal tract to the outside of the body. There are different types of stomas including ileostomies, colostomies, and urostomies. Ileostomies divert small intestine contents and have a liquid effluent that is discharged continuously. Colostomies divert large intestine contents and have solid, intermittent effluent. Stomas can be temporary or permanent depending on the clinical situation and are constructed in different ways including as an end stoma or loop stoma. Proper stoma care and use of appliances is important for managing stomas.




































































![Basics of Stoma and Management care[1].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/basicsofstomaandmanagement1-250417022629-8799f789-thumbnail.jpg?width=640&height=640&fit=bounds)























