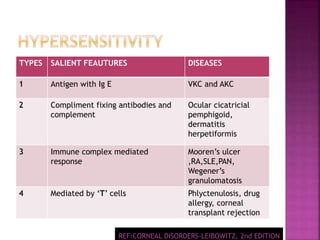
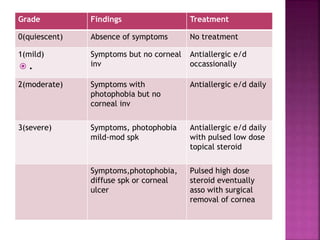
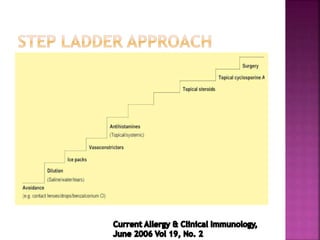
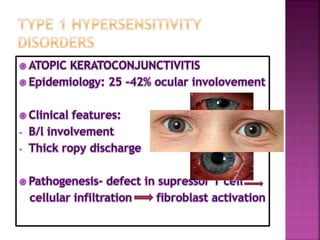
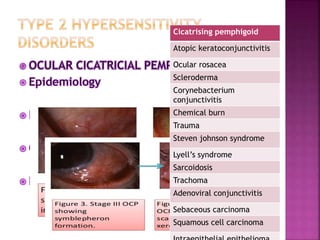
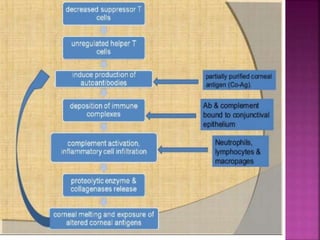
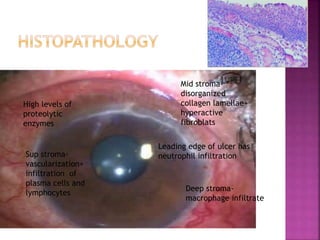
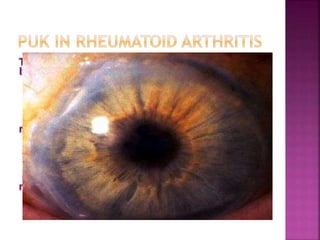
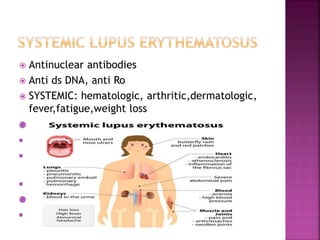
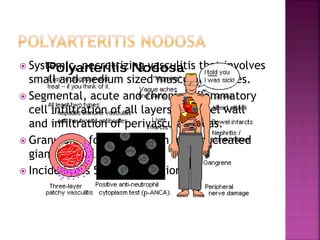
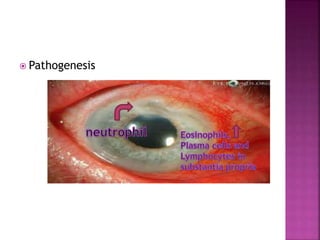
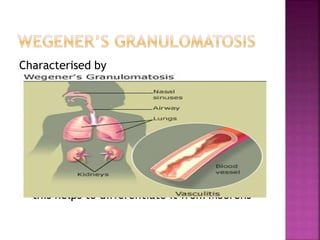
The document discusses the pathology and treatment of various corneal disorders, including Mooren's ulcer, atopic keratoconjunctivitis, and peripheral ulcerative keratitis. It highlights the immunological mechanisms involved, outlines clinical features, and suggests management strategies, including corticosteroids and surgical interventions. Additionally, it reviews the systemic conditions associated with these ocular diseases and their therapeutic approaches.