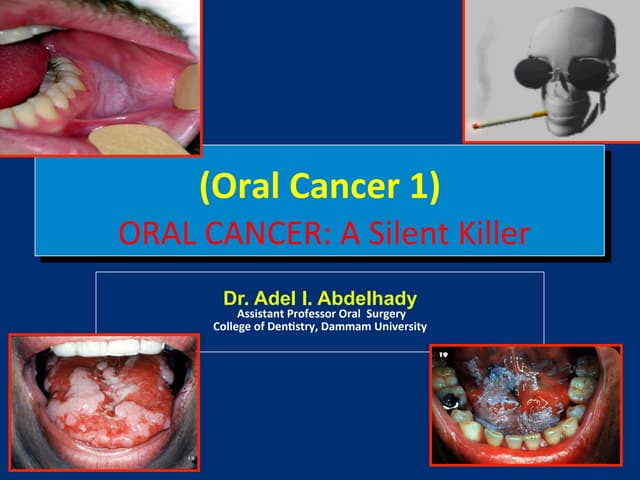
This document discusses oral squamous cell carcinoma, including its definition, risk factors, signs and symptoms, diagnosis, treatment, and prevention. Key points:
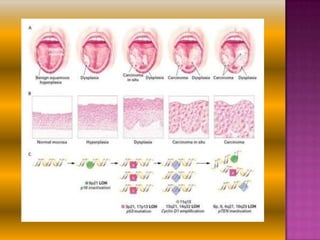
- It is a malignant neoplasm of the oral cavity epithelium capable of local growth and metastasis. Major risk factors include tobacco use, alcohol consumption, and HPV infection.
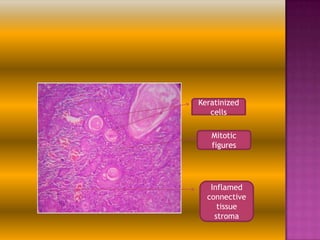
- Common symptoms are non-healing sores, lumps, pain or difficulty swallowing. Diagnosis involves biopsy and imaging tests. Treatment options are surgery, radiation, chemotherapy and rehabilitation.
- Prevention focuses on reducing risk factors through health education and discouraging behaviors like smoking, as well as early detection through screening to find cancer at earlier, more treatable stages.