Downloaded 383 times



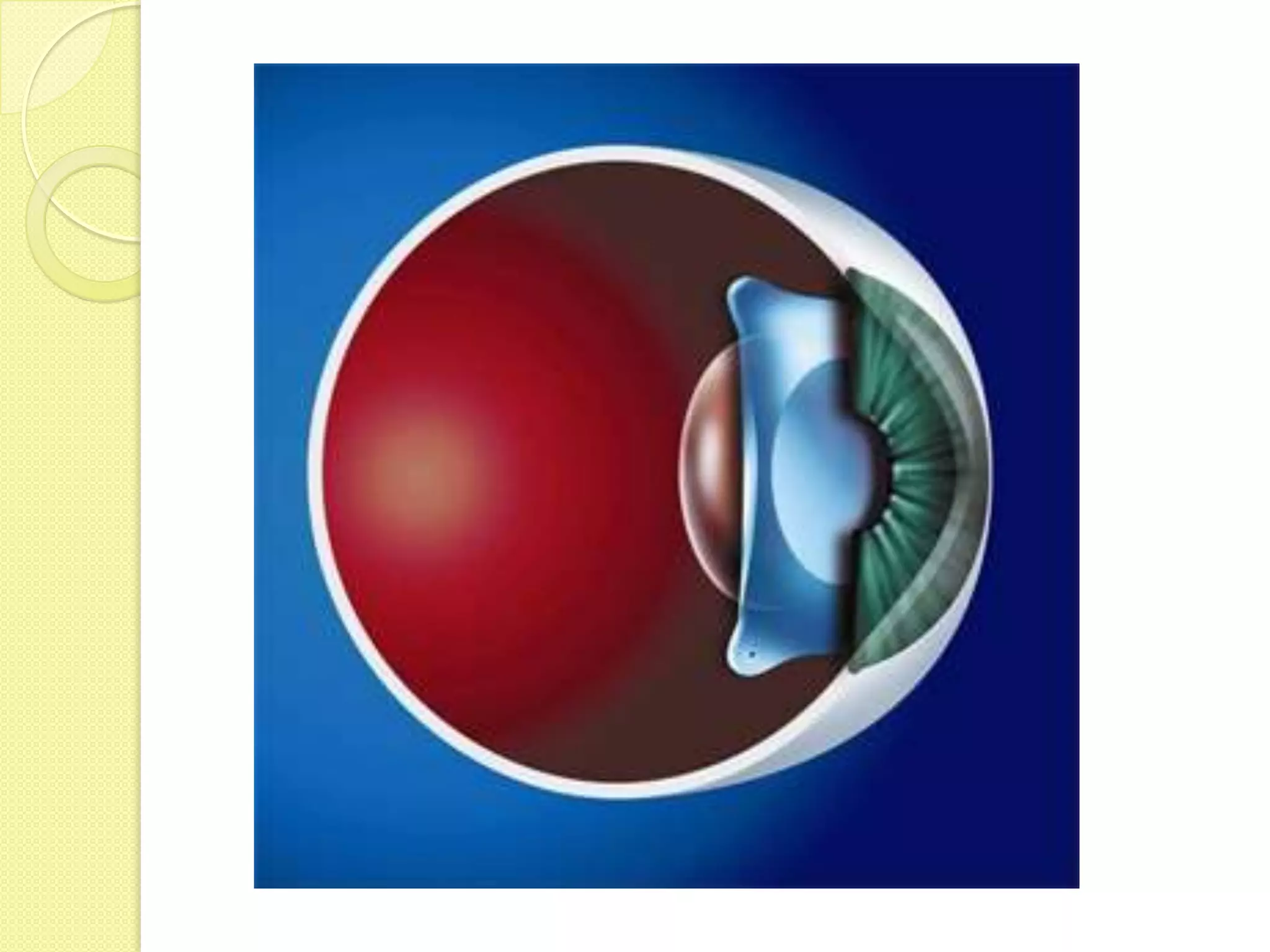











The Implantable Collamer Lens (ICL) is a soft, flexible, posterior chamber phakic intraocular lens made of collagen-copolymer material called Collamer. Studies have shown ICL implantation is safe and effective for correcting myopia between -3 to -25 diopters and astigmatism up to -6 diopters. It provides stable refractive results with few complications over 4 years. Toric ICL models were found to be superior to LASIK in safety, efficacy, predictability and stability for high myopic astigmatism. The procedure is reversible and preserves corneal tissue, reducing risks compared to LASIK.











































































































