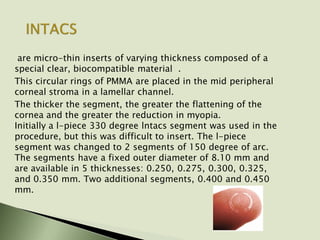
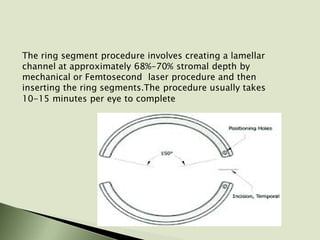
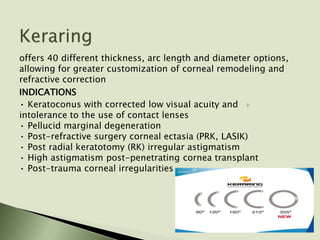
Intracorneal ring segments, such as INTACS, are thin plastic rings that are implanted into the corneal stroma to flatten the cornea and reduce myopia. They are placed in a lamellar channel using either a mechanical or laser procedure. Thicker rings provide greater flattening and myopia correction. Potential risks include visual disturbances and complications requiring removal. Intracorneal rings have been used off-label to treat conditions like post-LASIK ectasia and keratectasia with some success in improving vision.














































































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





