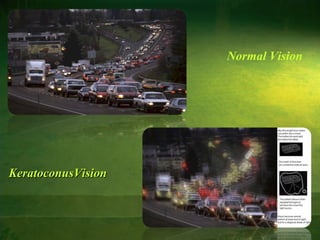
Keratoconus is a non-inflammatory condition where the cornea progressively thins and changes from a dome shape to a cone shape. It typically develops between ages 8-45. The cornea thins and breaks occur in the Bowman's layer and Descemet's membrane. Diagnosis involves examining for Fleischer's ring, Vogt's striae, and irregular topography. Mild cases are treated with glasses or soft contacts while more severe cases require rigid gas permeable contacts or surgical interventions like intracorneal ring segments, lamellar keratoplasty, or penetrating keratoplasty.