Downloaded 1,009 times
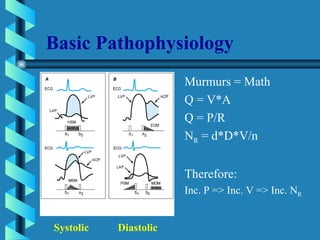

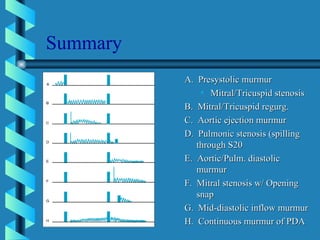

This document provides an overview of different types of heart murmurs: 1. It describes systolic murmurs which occur during ventricular contraction and can be early, mid, or late systolic. Common causes are aortic stenosis, mitral regurgitation, and mitral valve prolapse. 2. It also describes diastolic murmurs which occur during ventricular relaxation and include early diastolic murmurs from aortic regurgitation and rumbling mid to late diastolic murmurs from mitral stenosis. 3. Continuous murmurs that begin in systole and continue into diastole are also discussed, along with how to characterize location and timing of different murmurs.