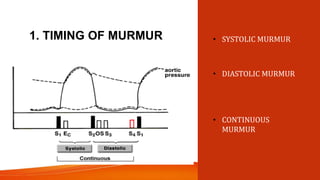
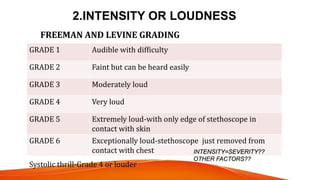
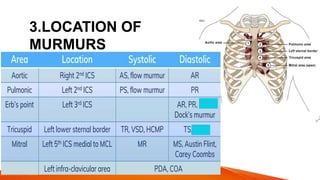
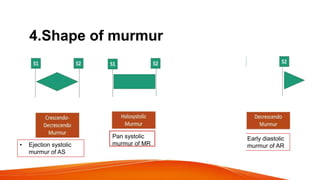
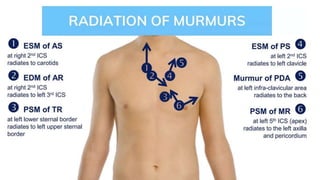
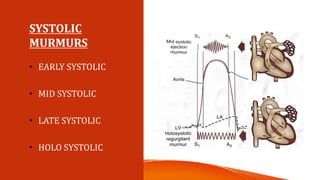
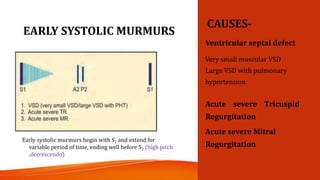
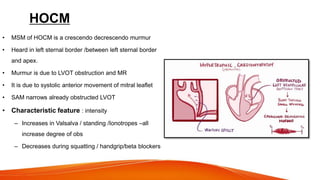
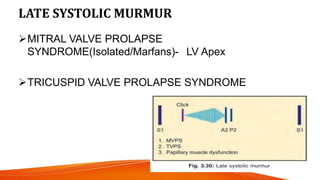
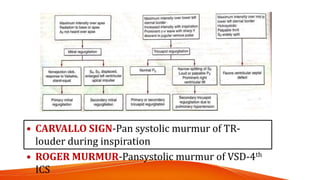
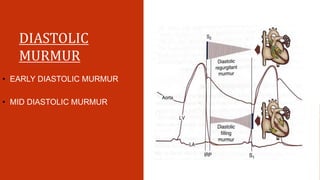
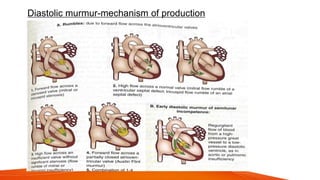
The document discusses the characteristics and classifications of heart murmurs, detailing the mechanisms behind their production, techniques for describing them, and various types of murmurs associated with different cardiac conditions. It emphasizes the timing, intensity, location, pitch, and configuration of murmurs, along with their clinical significance and diagnostic approaches. Additionally, the document covers a variety of specific murmurs related to conditions such as aortic stenosis, mitral regurgitation, and the physiological factors influencing murmur audibility.