Downloaded 586 times

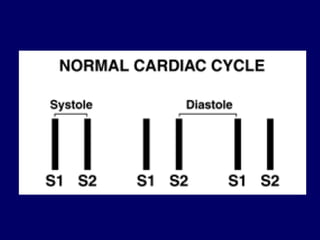
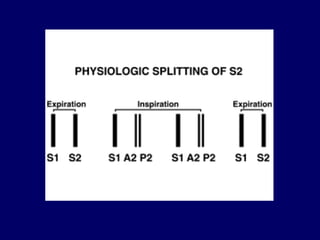
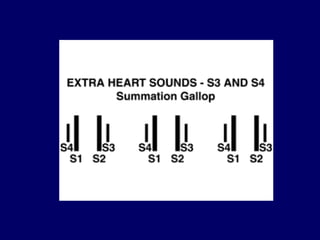
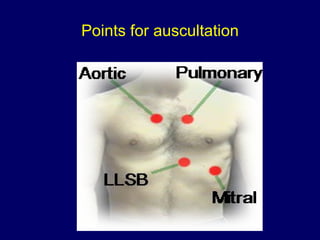
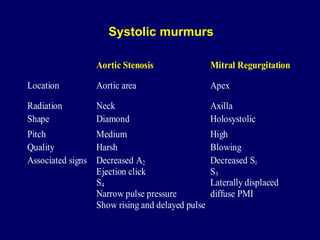
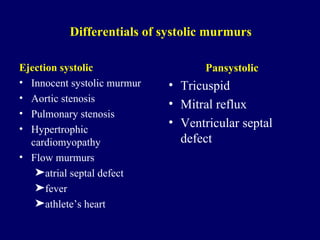
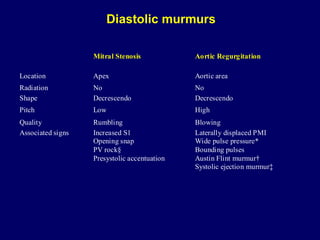

The document discusses auscultation of the cardiovascular system. It describes the normal heart sounds S1 and S2 and factors that can influence their intensity. Extra heart sounds S3 and S4 that indicate pathology are described. Points for auscultating murmurs are provided, including describing timing, location, radiation, duration, intensity, pitch and quality. Systolic and diastolic murmurs and their differentials are briefly discussed.



























































![[Int. med] heart murmurs from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/b29t6cwrtzwunmrfazue-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171700-lva1-app6891-thumbnail.jpg?width=640&height=640&fit=bounds)


























