Downloaded 2,874 times
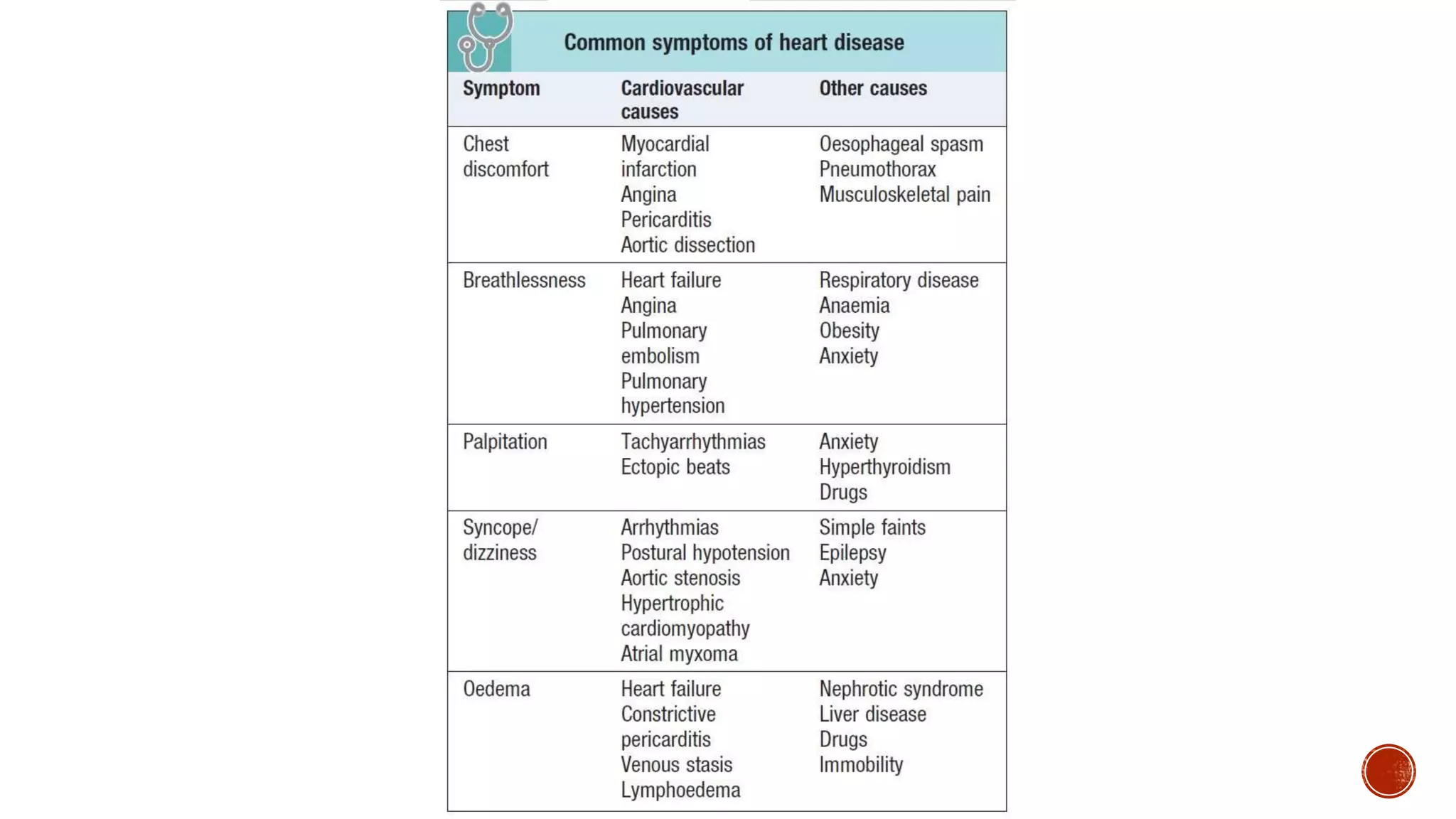
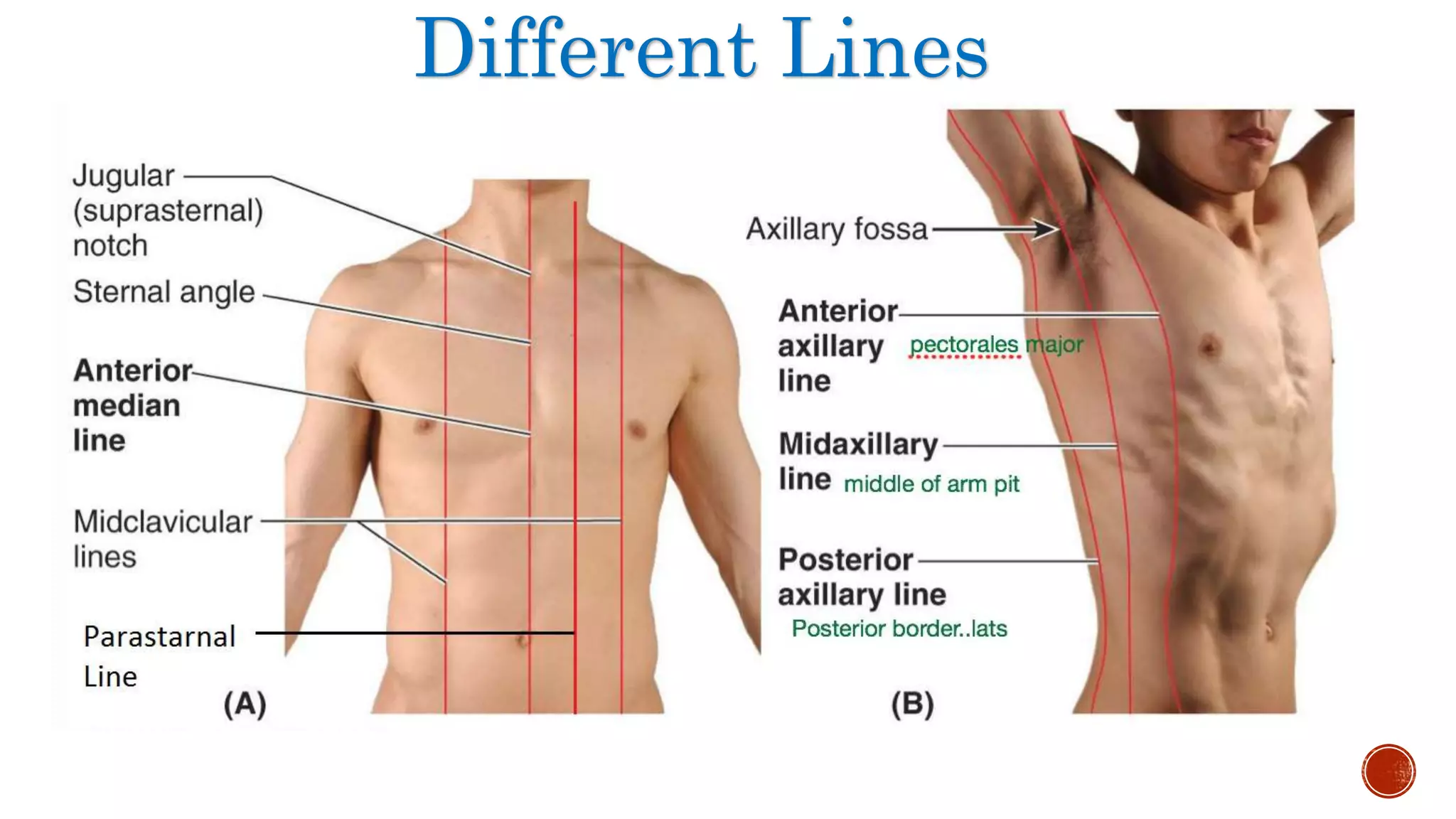



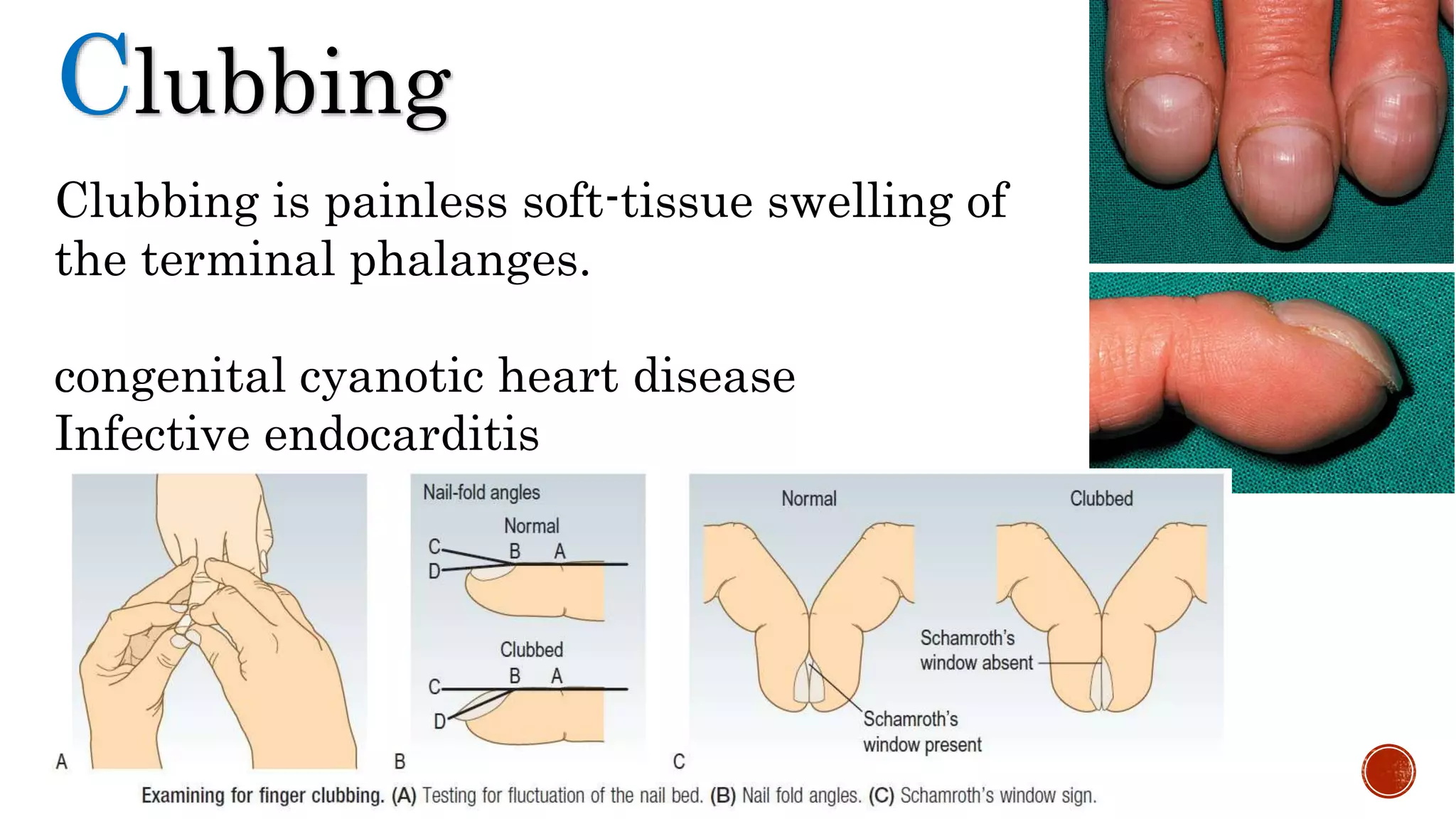
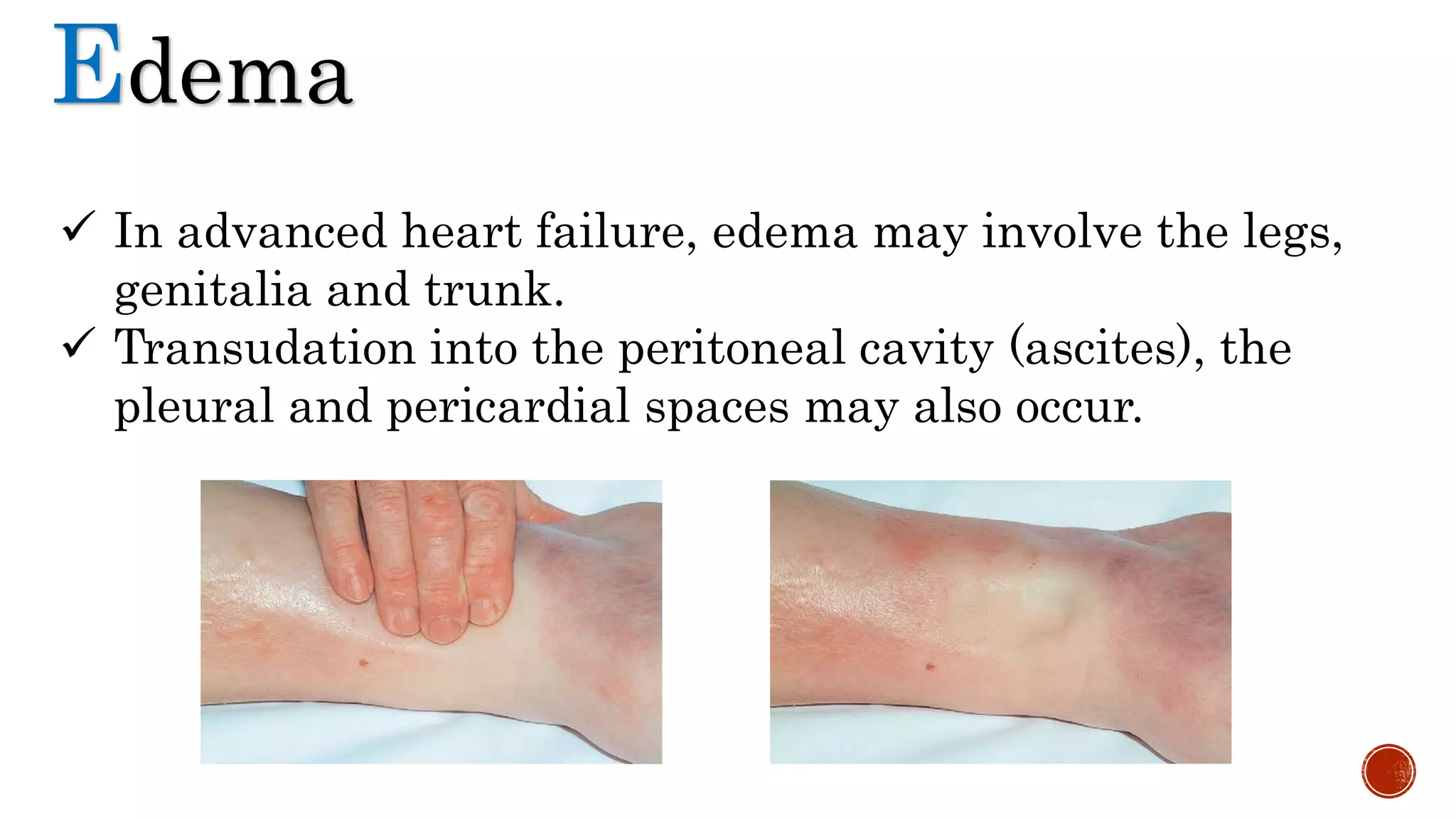







The document details the clinical examination of the cardiovascular system, covering aspects like general examination, neck vein assessment, precordium examination, and various heart sounds. It emphasizes the identification of symptoms such as pallor, cyanosis, clubbing, and edema, as well as techniques for inspecting, palpating, percussing, and auscultating the heart. The findings from the examination are summarized, indicating that the cardiovascular system of the subject is normal.










































































