Downloaded 396 times
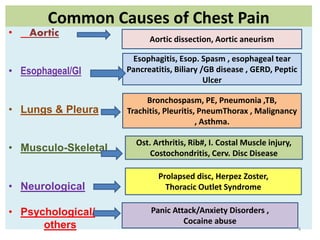
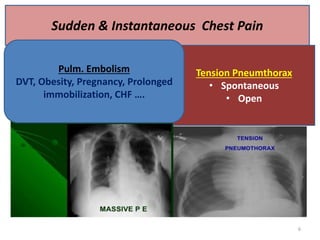
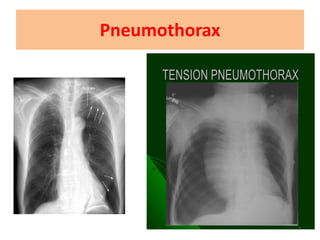
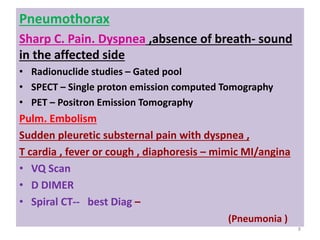
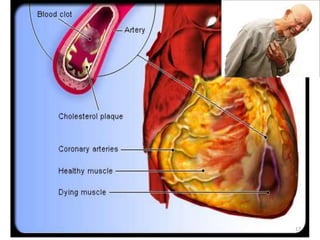
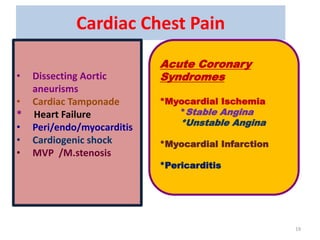
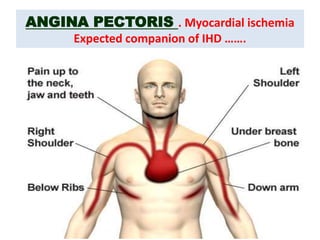
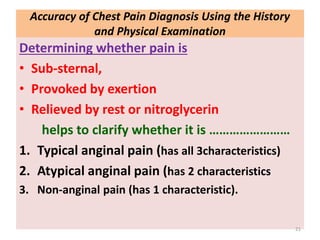


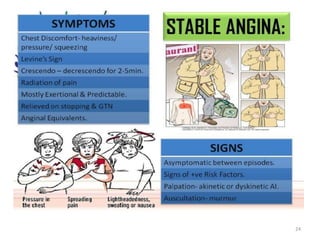
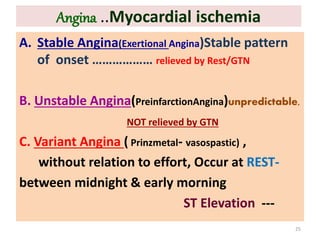
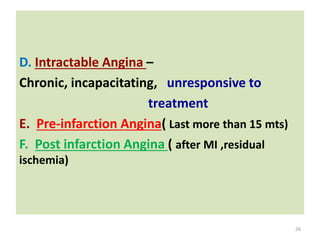
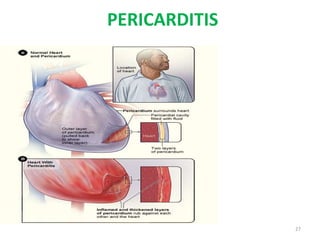
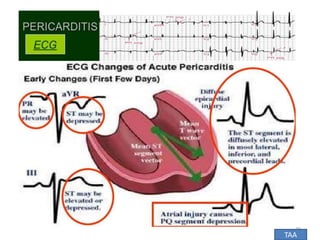
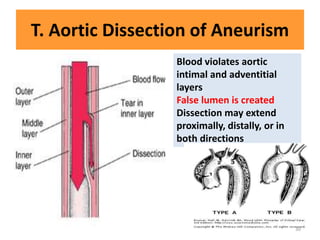

This document discusses the differential diagnosis of chest pain by describing various cardiac and non-cardiac causes. It outlines key factors in the history and physical exam that can help determine if chest pain is typical angina, atypical angina, or non-anginal. Common cardiac causes discussed include acute coronary syndromes, aortic dissection, and pericarditis. Common non-cardiac causes discussed include pulmonary embolism, pneumonia, gastrointestinal issues like pancreatitis and peptic ulcer disease. Diagnostic tests for different conditions are also mentioned.























































![[Int. med] chest pain 3rd year class](https://cdn.slidesharecdn.com/ss_thumbnails/int-150502144317-conversion-gate02-thumbnail.jpg?width=640&height=640&fit=bounds)
![[Int. med] chest pain 3rd year class from SIMS Lahore](https://cdn.slidesharecdn.com/ss_thumbnails/zkh5x8lztsickjayhfry-signature-b01672da1ecf8b94befb115319b147a085de390b8cb403389bce6c156545fbb5-poli-150815171705-lva1-app6892-thumbnail.jpg?width=640&height=640&fit=bounds)


















































