Downloaded 61 times

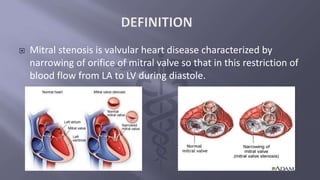













Mitral stenosis is a valvular heart disease characterized by the narrowing of the mitral valve orifice, often resulting from rheumatic fever, which can take decades to develop. Clinical features include dyspnea, cough, and signs of pulmonary edema, with diagnostic investigations such as echocardiography and electrocardiograms revealing atrial hypertrophy. Treatment options include medications, valvuloplasty, and mitral valve replacement, alongside a structured physiotherapy regimen for patients with operative conditions.

















































































