This document provides an examination of the cardiovascular system. It begins with a general examination including vital signs. It then discusses signs such as pallor, cyanosis, clubbing, and edema. The document examines the pulse, blood pressure, jugular venous pressure, and auscultation of heart sounds. It provides details on normal and abnormal findings for each of these exam components. The document concludes with an examination of peripheral pulses and abnormalities of the jugular venous pulse.



![Central Cyanosis :-
Causes:-
A] ↓sed arterial O2 saturation :-
a) High altitude ( d/to ↓sed atm pressure),
b) V/P mismatch,
c) Anatomic shunts ( desaturated bld bypassing lungs )-
1) Cyanotic CHD,
2) Pulm AV fistula,
d) Hb with low affinity for O2.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-5-2048.jpg)
![B] Hb abnormalities :-
a) Methhaemoglobinemia (>1.5g/dl) –
1) Hereditary,
2) Aquired – Nitrates, sulphonamides.
b) Sulfhaemoglobinemia (>0.5g/dl),
c) Carboxyhaemoglobinemia (smokers).
• In Meth-Hb-nemia – Pt’s bld remains brown after exposing to fr
air.
But in cyanosis d/to reduced arterial O2 saturation;- Pt’s bld tur
red on exposure to air.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-6-2048.jpg)
![Peripheral cyanosis :-
Causes :-
A] Reduced CO ( Reduced flow causing more O2 extraction ),
B] Cold exposure,
C] Arterial/venous obstruction,
D] MS – cyanosis over malar area produces malar facies/ malar flu](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-7-2048.jpg)
![Differential cyanosis :-
Causes :-
A] Cyanosis seen only in LLs - PDA with Pul HTN with R→L shunt
B] Cyanosis seen on,y in ULs – --”-- & Transposition of grt vessels](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-8-2048.jpg)



![• Theories of clubbing :-
A] Neurogenic – Vagal stimulation →vasodilation →clubbing.
B] Humoural – GH, PTH, Oestrogen, PGs, bradykinin →vasodilata
C] Ferritin - ↓sed ferritin →Dilatation of AV anastomoses & hypertro
D] Persistent hypoxia → opening of AV fistulae of terminal phalynx
E] PDGF – Released 2ndary to infn in body →vasodilation →clubb
Latest & most accepted theory of clubbing.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-14-2048.jpg)
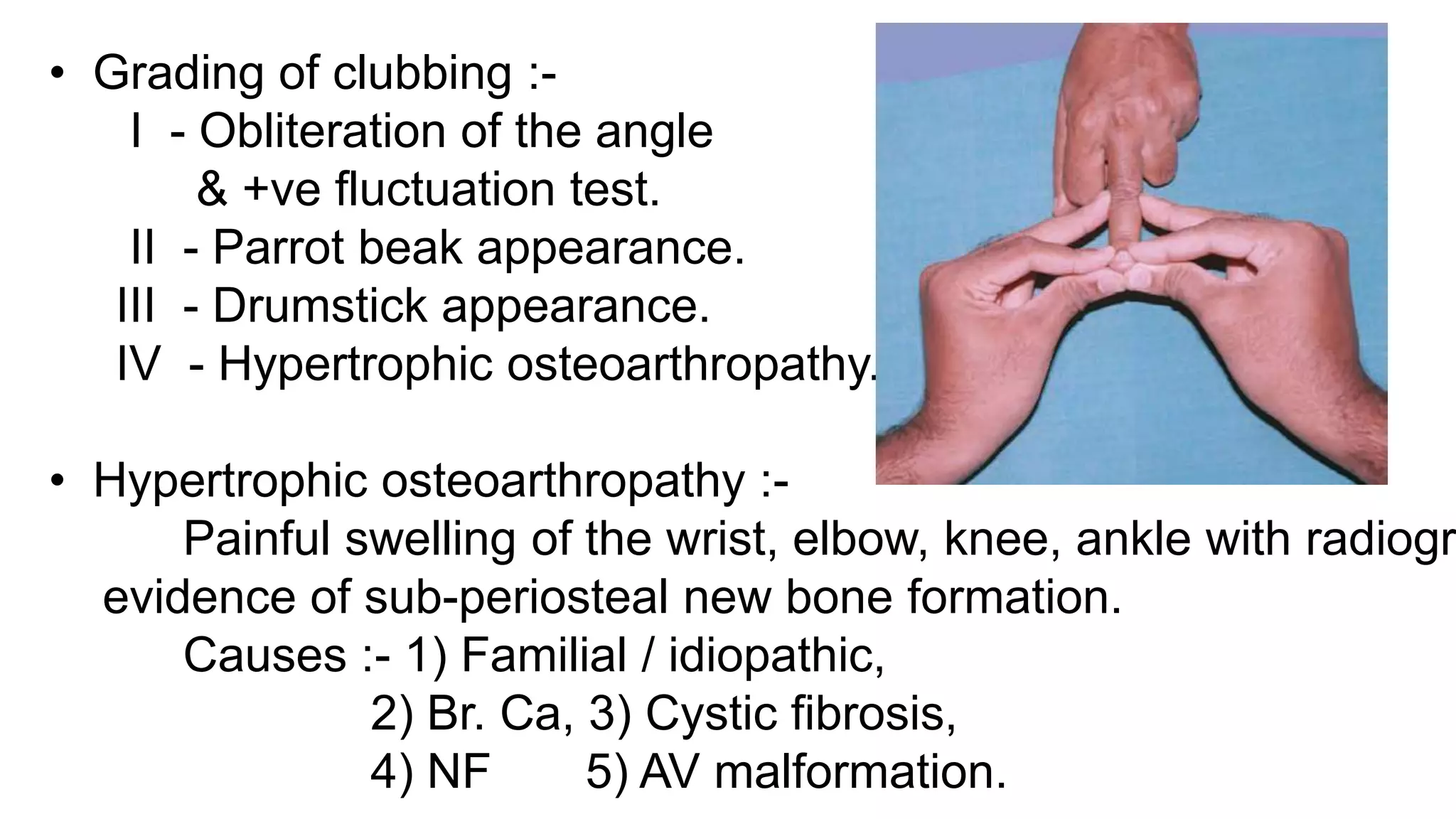
![• Causes of clubbing :-
A] Congenital / familial,
B] Aquired – Tophaceous gout,
Local injury,
Sarcoiodosis,
Hemiplegia.
C] Pulm/ Thoracic causes – Br. Ca, Metastatic lung ca, chronic br
Suppurative lung d/ses;- cystic fibrosis,
lung abscess,
empyema,
bronchiectasis.
Interstitial lung d/ses,
Long standing pulm TB,](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-15-2048.jpg)
![D] Cardiovascular causes - Cyanotic CHDs,
Infective endocarditis,
Atrial myxomas,
E] GI causes – Liver cirrhosis,
Ulcerative collitis,
Crohn’s d/s,
GI malignancy.
F] Miscellaneous – Syphilis,
Acromegaly,
Thyrotoxicosis.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-16-2048.jpg)
![Oedema :-
• S.C. edema which pits on pressure – cardinal feature of CHF.
• Pressure appd over bony prominences.
• D/to H2O & Salt retention by kidneys.
• 2 major mechanisms :-
I] CHF
↓
Hypotension
↓
Reduced renal perfusion
↓](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-17-2048.jpg)
![Sympathetic activation & Ang-II production
↓
Preglomerular arteriolar constriction
↓
Reduced glomerular filtration
↓
Reduced Na+ delivery to nephron
II] Increased Na+ reabsorption from nephron
↓
More Imp mechanism.
Early heart failure – Na+ reabsorption mainly from PCT.
As HF worsens;- Na reabsorption also from DCT & CT
d/to activation of R-A-A system.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-18-2048.jpg)





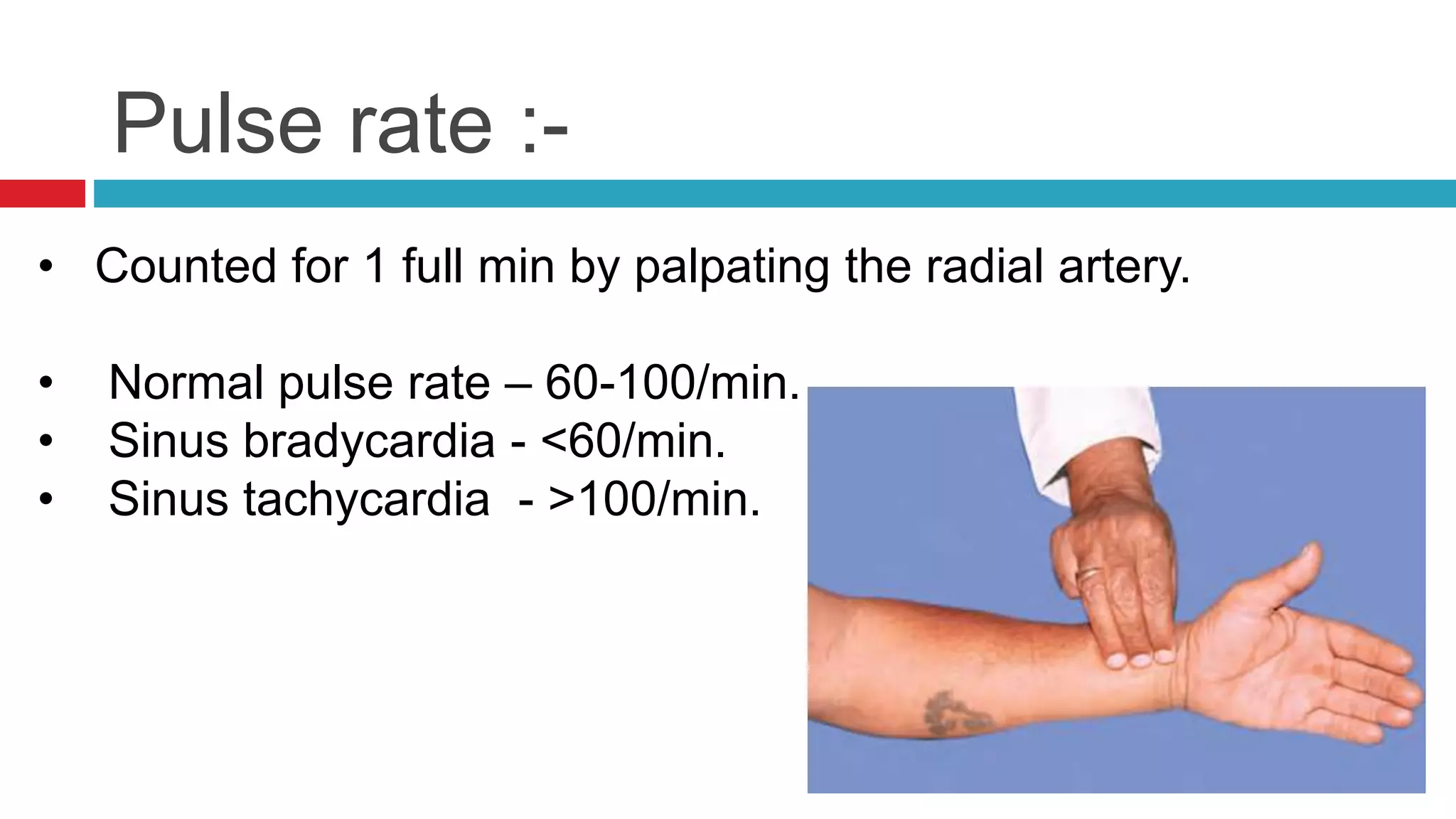

![Pulse rhythm :-
• Normal sinus rhythm - Regular
• Young patients – phasic veriations d/to “Sinus arrhythmia”.
• A] Regularly irregular rhythm –
Atrial tachyarrhythmias with fixed AV block,
ventricular bigemini, trimgemini.
• B] Irregularly irregular rhythm –
Atrial / ventricular ectopics,
AF,
Atrial tachyarrhythmias with variable AV block.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-28-2048.jpg)

























![Abnormalities of JVP :-
•A] a wave abnormalities :-
1) Absent a wave – AF.
2) Prominent a wave – PS, Pulm HTN, TS.
3) Cannon/Giant a waves - CHB, Multiple ectopics.
•B] Abnormalities of x descent - 1) Prominent – constr. Pericarditis
2) Absent – TR (instead may be +ve)
•C] Prominent v wave – TR.
•D] Absent y descent – Cardiac tamponade.
•E] False rise in JVP – Polycythemia vera (↑sed bld vol)
Sympathetic stimulation d/to pain, anxiety,etc](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-60-2048.jpg)






![Visible pulsations :-
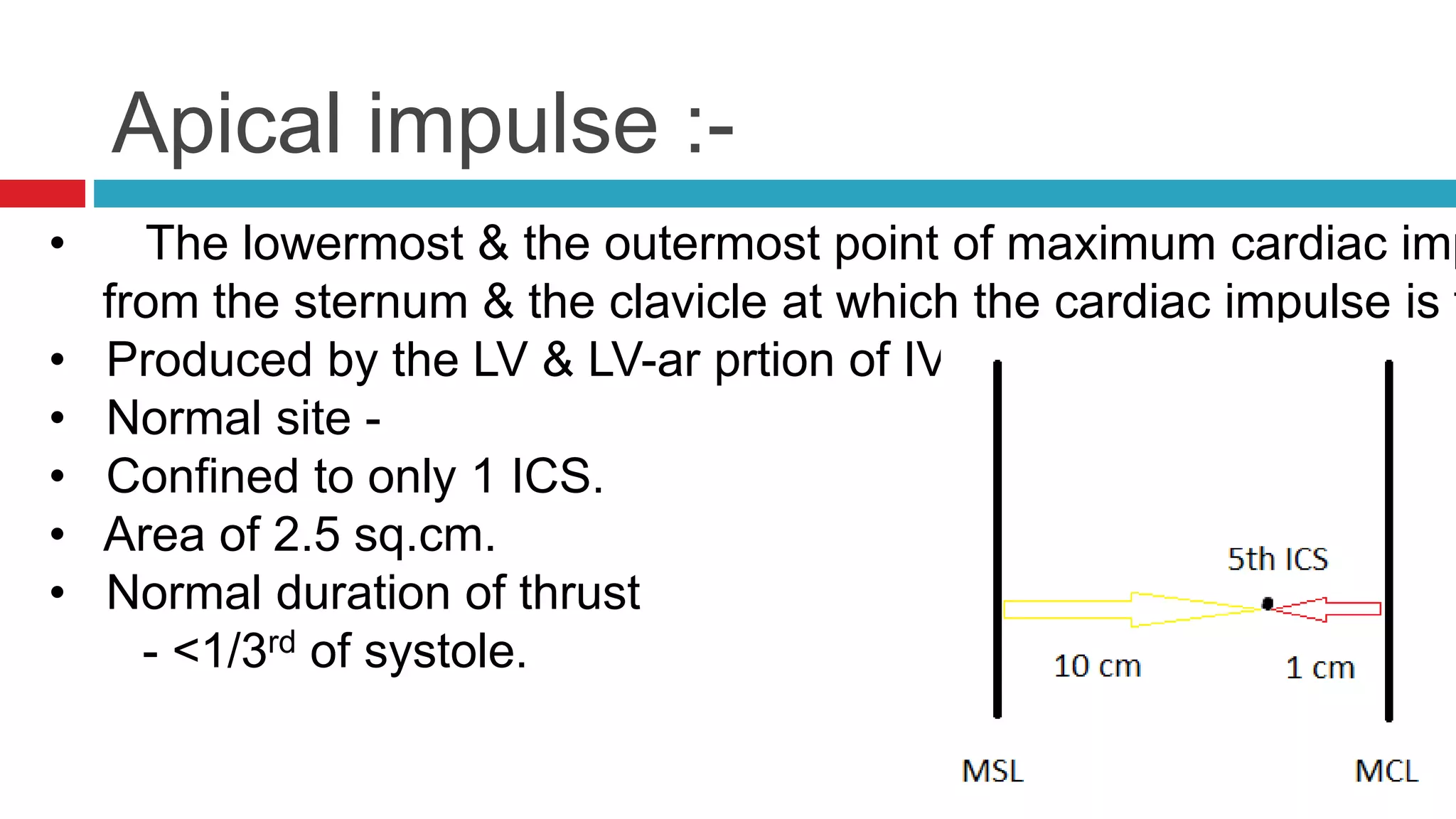
• A] Apical impulse – Lowermost & outermost pt of max.m impulse
sternum & clavicle at which cardiac impulse can be
• B] Carotid pulsations – 1) Hyperdynamic states,
2) AR,
3) CoA,
4) Systemic HTN.
• C] Suprasternal pulsations – 1) AR, 2) CoA,
3) Thyrotoxicosis.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-69-2048.jpg)
![• D] L parasternal pulsations – 1) RVH,
2) MR.
• E] Supraclavicular pulsations – AR.
• F] Epigastric pulsations – 1) AR,
2) RVH,
3) Hepatic pulsations (R lobe of liver),
4) Tumour/nodes overlying aorta.
• G] Hepatic pulsations – 1) TS,
2) TR,
3) AR.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-70-2048.jpg)








![• A] Carotid thrill/ Carotid shudder :- AS
• B] Aortic thrill :- Systolic – AS
Diastolic – Acute Severe AR,
Syphilitic AR,
• C] Pulmonary thrill :- Systolic – PS, ASD.
Continuous – PDA, Rupture of sinus of valsa
• D] L lower parasternal thrill :- VSD.
• E] Apical thrill :- Systolic – MR.
Diastolic – MS.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-81-2048.jpg)

























![Named murmurs :-
• A] Aortic valve –
• Gallavardin phenomenon Austin-Flint murmur
↓ ↓
The Harsh noisy component of Low-pitched rumbling mid-di
ESM of AS, best heard at the apex,
Which is best heard at the in severe AR.
R sternal border, &
Radiated to the neck.
• Cole-cecil murmur :- Murmur of AR well heard in axilla.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-111-2048.jpg)
![• B] CAREY COOMB’s Murmur :- Short, mid-diastolic murmur
best heard at the apex in cases
with MS in Acute RHD.
• C] Graham Still murmur :- High-pitched, Early diastolic murmur,
best heard at the left sternal border 2nd IC
during expiration in PR.
• D] Carvallo’s sign :- Pan-systolic murmur of TR,
best heard in tricuspid area,
which becomes louder during inspiration.
• E] Gibbson murmur :- Continuous machinery murmur of PDA.](https://image.slidesharecdn.com/cardiovascularsystemexamination-170514182612/75/Cardiovascular-system-examination-112-2048.jpg)



















































































