Downloaded 46 times

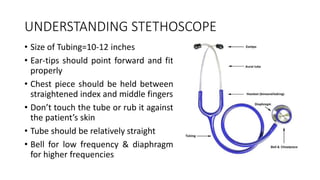
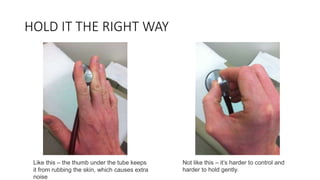
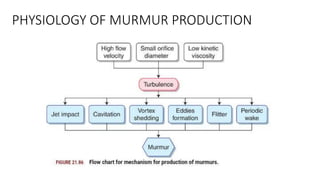
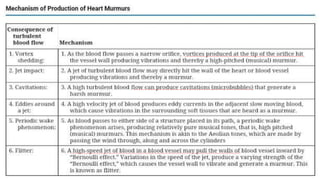
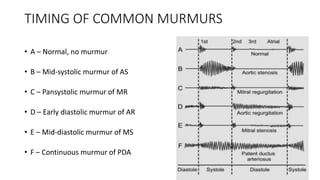
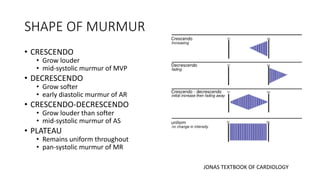
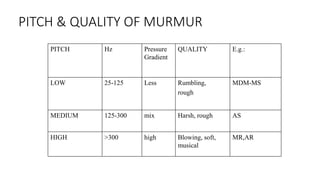
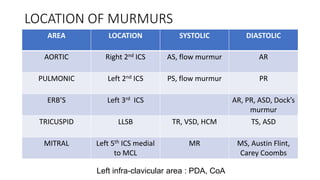
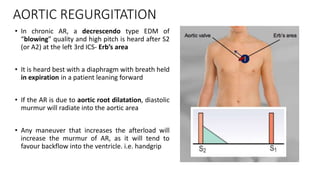
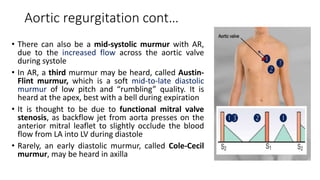
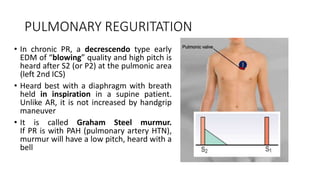
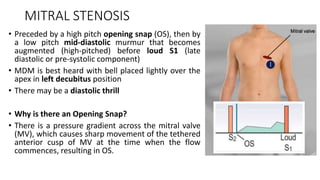
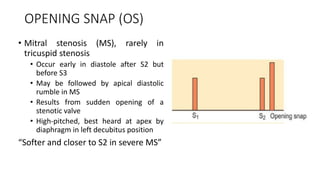
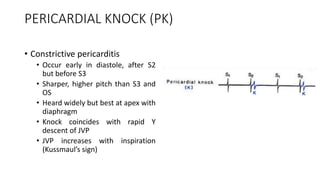
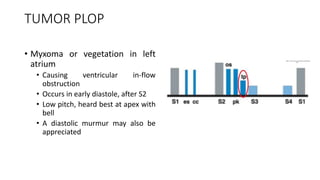
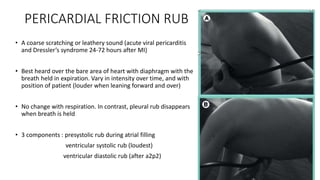




1. The document describes how to properly hold and use a stethoscope to listen to heart sounds and murmurs. It discusses positioning the ear tips, chest piece, and avoiding touching the tubing to reduce extra noises. 2. Key aspects of cardiac murmurs are defined, including their timing within the cardiac cycle, causes, pitch, quality, location, and how they change with maneuvers. Common murmurs from conditions like aortic stenosis, mitral regurgitation, and ventricular septal defects are detailed. 3. Dynamic auscultation, or how murmurs change with respiration, body position, and other stresses, is an important part of diagnosis. Variations























































































